Chapter 1: Nose Reshaping: An Overview
Chapter 2: Choosing a Cosmetic Surgeon
Chapter 3: Your Consultation
Chapter 4: Preparing for Your Rhinoplasty Surgery
Chapter 5: Your Rhinoplasty Procedure
Chapter 6: After Your Rhinoplasty Procedure
Chapter 7: Revision Rhinoplasty
In Closing
Patient’s Guide Appendix
I owe a special thanks to my family for their love and support.
I owe special thanks to my mentors, colleagues and friends: M. Eugene Tardy Jr., MD FACS, Dean M. Toriumi MD, Robert W. Cantrell MD, Paul A Levine, Charles W. Gross, Richard F. Edlich, Stephen S. Park, and others for their mentorship, collegiality and friendship.
Chapter 1: Nose Reshaping: An Overview
What is Rhinoplasty?
Rhinoplasty is surgery to reshape the nose. It is a very popular procedure – in fact, over 300,000 Americans undergo this operation each year! Common requests include making a nose smaller, reducing the bridge of the nose, narrowing the nose, making changes to the nasal tip, lifting a droopy nose, revising a previous rhinoplasty and others.
What bothers one person about their nose may not bother another person. Still, most rhinoplasty patients know what they do not like about their nose. If you do not like the way your nose looks, if you are willing to undergo a surgical procedure, and if you are in good physical and mental health, then you may be a good candidate for rhinoplasty.
Types of Rhinoplasty – Functional v. Cosmetic, Open v. Closed
Question: Will insurance cover my surgery?
Answer: If your requests are functional (for example, you cannot breathe through your nose, or if you suffered a relatively recent, documented nasal fracture), many insurance companies will cover the part of the surgery that is required to correct these problems.
However, any requests relating to a change of appearance are generally not covered by insurance companies, and do require a cosmetic surgery fee.
Question: How do you do a rhinoplasty?
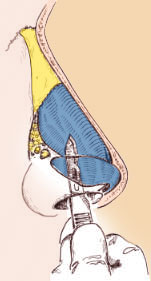
Answer: The two general types of rhinoplasty are the endonasal (“closed” rhinoplasty – all incisions hidden inside the nose) and the external (“open” rhinoplasty – all incisions EXCEPT one small incision are inside the nose.) In open rhinoplasty there is one small incision across the columella (the skin between the nostrils). This incision is generally extremely difficult to see, and is only about 3 mm (1/10th of an inch) long!
I perform both closed and open rhinoplasty. I have written a recent scientific article on this subject, entitled “Open Versus Closed Rhinoplasty.” Let me summarize the conclusions for you here: The decision on which technique to use depends on technical considerations with respect to the patient’s specific anatomy and his or her cosmetic requests, and also depends on physician experience with both techniques.
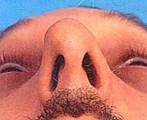
This patient had an open rhinoplasty 4 years ago. Look at his base view – see the incision?


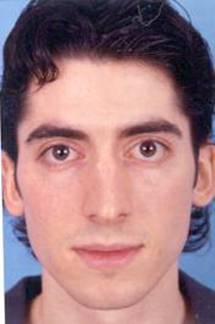


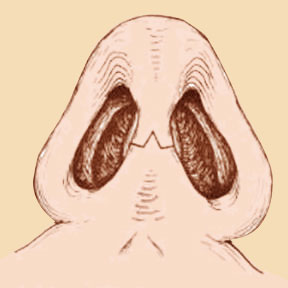
The patient below had a closed rhinoplasty. His incisions were all on the inside of his nose:


In my experience, the closed approach is better for some noses, while the open technique is better for others. For example, in my practice the patient who requests simply a small hump removal may undergo endonasal rhinoplasty, while the patient with a severely twisted nose often requires – for technical reasons – an open approach for the best result. The approach I pick is based on what I think will provide the best outcome for you, and based upon our detailed discussion about the technical aspects of your procedure.
The female patient shown here underwent an open approach because her nose was twisted and needed straightening. If she had only needed profile changes, I might have undertaken a closed approach. Can you tell that her surgery was open?!




Fortunately, there are no major disadvantages to either approach. However, each approach has special advantages for specific situations. Since every nose is different and has unique surgical requirements, I discuss the options with each patient and am happy to describe my surgical plan in detail.
Ethnic Rhinoplasty
I perform rhinoplasty on all ethnic groups. The categories of ethnic groups include Caucasian, Asian, African-American, and Hispanic. Please see the Ethnic Rhinoplasty Section for more detailed information.
Surgical Philosophy
You should understand the surgeon’s philosophy. First, you should find a surgeon who has a philosophy about rhinoplasty! In my opinion, a surgeon who philosophically takes a conservative approach to rhinoplasty is preferable. The surgeon’s approach should be one in which he or she avoids over-aggressive resection maneuvers, focuses on maintaining structural support, and seeks a natural “un-operated” appearance.
Limitations of Rhinoplasty – Realistic Expectations
Rhinoplasty can change your appearance, and to a certain degree it can change the way you feel about yourself and how others relate to you. But, rhinoplasty will not “change your life.” The patient must have a realistic appreciation of the physical and psychological changes that can be achieved, and must have a realistic appreciation of the potential functional, cosmetic, and psychological risks. We will discuss this more below.
Are you a Good Candidate? Or a Bad Candidate?
If you do not like the way your nose looks and are willing to undergo a surgical procedure, and if you are in good physical and mental health, then you are eligible for a rhinoplasty consultation. During your consultation, I will talk with you in detail and examine you. I will also undertake computer imaging so that I can understand your surgical goal. Then, I will explain my expectations for your surgery and will let you know if I think you are a good candidate.
All patients must understand that surgery is an art and a science. Cosmetic surgical procedures have been repeated successfully countless times and are dependable when executed by skillful, experienced surgeons. Despite the best efforts of a talented surgeon, a complication can still occur. Although most complications are relatively minor and correctable, more serious, debilitating, and un-correctible complications do occur . There is no way to be certain that a complication will not occur. Plastic surgery is a combination of art and science, and as such can be subject to unpredictables – usually (but not always) minor and correctible in nature. A patient undergoing rhinoplasty must understand this and accept the possibility of a complication.
Once you have chosen a surgeon, have a candid discussion with the surgeon regarding your goals and expectations of surgery. A discussion of the potential complications is critical, so that you understand the risks of a complication.
Age Requirements
Most rhinoplasty surgeons prefer to wait until an individual has completed his or her growth spurt. This means age 15 or 16 for girls, and a little later for boys. Of course, this is a generalization: it is very important to consider the individual’s emotional and social maturity level and to make sure that he/she really wants a rhinoplasty.
If you are in good physical and mental health, age is not usually the over-riding factor. Rhinoplasty in the 40s and 50s is relatively common. Perhaps the oldest patients for whom I have performed a rhinoplasty has been for an occasional patient in their 70s.
Emotional Health
It is important that you are in strong emotional health. If you generally happy in life but simply do not like the way your nose looks, and are interested in a cosmetic improvement, then you are probably a good candidate for rhinoplasty consultation.
However, if you are in a stressful period of your life – a divorce, personal or financial tragedy, this is a bad time to have cosmetic surgery. If you believe that having a nose job will change your life, improve a relationship or a marriage, etc… then you should not have this surgery. If you have a psychiatric illness, this illness should be under good control, and you should seek advice from your psychiatrist before giving this further consideration.
Physical Health
If you are in a general state of good health, such that a 2 hour anesthesia and surgery does not present a greater than normal risk, then you probably are eligible for rhinoplasty from the physical health perspective.
However, if you have serious acute or chronic illnesses, you should probably only have surgeries that are absolutely necessary!
Smoking
Smoking delays healing and increases the risk of poor healing and infection. Smokers should be prepared to quit for at least 3 weeks before and after surgery.
And, if you are serious about rhinoplasty, why not use this as an excuse to quit!
Chapter 2: Choosing a Rhinoplasty Surgeon
There is both a science and an art to rhinoplasty.
It takes skill and experience to be able to examine a nose and deduce the anatomy – why the nose looks like it does.
Then, it takes skill and experience to decide on the surgical techniques that will give the best chance for success.
Just like artists, athletes, and virtually all professions in life, some surgeons are simply better at rhinoplasty than others. It is not enough to have a good forehand, backhand and serve – the surgeon must string them all together for a winning point, game and match!
But, how do you find the right surgeon?
There is no shortcut to choosing a rhinoplasty surgeon. You have to do your own research. A referral from a doctor, an aesthetician, from a friend/patient, or by “word of mouth” can help, but I would not suggest relying on them completely.
There are certain critical facts about the doctor and practice, such as how often they perform rhinoplasty, that you should know before undergoing surgery. There are a number of credentials that a doctor must have to perform facial plastic surgery, and there are a number of specialties within the field. Knowing which one (or ones) your doctor specializes in will help you to make an educated decision. For help finding a surgeon in your area, the American Board of Facial Plastic and Reconstructive Surgery (ABFPRS) may be a useful resource. The ABFPRS qualifies facial plastic surgeons. The American Board of Otolaryngology also includes extensive training in facial plastic surgery, and is recognized to qualify facial plastic surgeons by the ABMS.
Once you find a doctor whose credentials you are satisfied with, you should meet with him or her to see if you feel comfortable. The doctor should be able to explain the procedure to your satisfaction, and instill confidence in you. You may wish to inquire into their status within the community, hospital and/or special societies. It is important to establish that the doctor has a special expertise in rhinoplasty.
It is important that you see examples of the surgeon’s rhinoplasty results. Many surgeons show these on their websites, and typically have them available in the office as well. This is not a guarantee of success, but it can give you an idea about the surgeon’s personal aesthetic and an idea about his ability. If you do not like the After Pictures that the surgeon has shown, pictures that he is proud of, then that is probably the wrong surgeon for you!
The web chatrooms may or may not help. Some patients have found them helpful, while some patients have said they can be misleading sometimes.
Your initial research may help you narrow your search down to a few surgeons, or to one surgeon. But, there is still the office consultation, the “Interview.” In the office, you will get a gut reaction. Do you like the surgeon? Does he seem to have a passion for the operation? Does he take the time to explain the surgery, in detail? Does he listen to what you want, or does he tell you what he wants to do?
In the end, there is no guarantee. You cannot negotiate away the risk of surgery. If you are looking for a new car and do good research, most tend to arrive at the same great car companies that make great cars. But, occasionally, every great car company (like Lexus, or Mercedes, or Porsche) turns out a lemon!
If you do the right research, you should be able to find a “great surgeon.” But, this assumes that your research is good! And, remember, even the best surgeon has a bad outcome every once in a while!
Surgeon Qualifications
Training and Education
There are different paths to becoming a rhinoplasty surgeon. The 2 most common are described here:
After medical school, some surgeons do a 5-6 year residency in Otolaryngology (Ear, Nose, and Throat). This training alone qualifies these surgeons under the American Board of Medical Specialties (ABMS) guidelines to perform rhinoplasty. However, some surgeons do an additional year of training in Facial Plastic and Reconstructive Surgery. These surgeons spend an extra year of training focusing on facial plastic surgery including rhinoplasty. In general, these surgeons are more likely to perform rhinoplasty on a more frequent basis.
Some surgeons spend their 5-7 years after medical school doing a general surgery residency. This training alone does not qualify these surgeons to perform rhinoplasty. These surgeons, if interested in performing plastic surgery, undertake an additional 2-3 years of training in plastic surgery, in which they focus on plastic surgery throughout the body and including the face. This training qualifies them to perform rhinoplasty under ABMS guidelines.
There are other other surgeons who perform rhinoplasty as well. However, the majority of rhinoplasty in this country is performed by surgeons with the training described above.
Licensure
State Licensure is a prerequisite to practicing medicine in every state of the United States. It is against the law to practice medicine in a State without licensure in that state. We recommend against surgery in the United States by any surgeon who is not licensed in their state.
Board Certification
Board Certification is an important aspect of choosing a surgeon. What does board certification mean? What exactly is a “board?”
A “board” is an organization that oversees an evaluation process. To be board certified means only that an individual has met all of the training and practice requirements put forth by that particular board.
The “main” board of all medicine in the United States is the ABMS, or American Board of Medical Specialties. This central board gives their seal of approval to many other certifying boards. Dr. Becker is board certified in the performance of facial plastic and reconstructive surgery by the American Board of Otolaryngology, an ABMS board and in fact one of the original ABMS boards. Dr. Becker is also certified by the American Board of Facial Plastic and Reconstructive Surgery. The ABFPRS is the only board that certifies surgeons exclusively for plastic surgery of the face.
Additional information about these boards is in the Appendix.
Experience in the Surgery
Experience begins in residency training. If the surgeon went to a training program where his plastic surgery teachers were world famous experts in facelift surgery, but only did an occasional rhinoplasty, that won’t help you very much!
Remember, just because a surgeon is good at one thing doesn’t mean he is good at another. A revision patient of mine told me that his mother had a facelift from a surgeon, and the result was great. When she asked him who would be a good surgeon to do her son’s rhinoplasty, he answered, “Me!” Unfortunately, he was better at facelifts!
Surgeons tend to have a “favorite” operation, one that they seem to have a passion or a knack for. This is something to keep in mind.
Does your prospective surgeon do a lot of this surgery? Who were his teachers – were they skillful and/or renowned rhinoplasty surgeons? Is your prospective surgeon active in their society, and up-to-date with the latest thinking on the subject? Are they teachers of their craft?
The Surgical Center
The Surgical Center should be an Accredited Surgical Center. A hospital-based surgery center is the most common.
Some surgeons perform surgery in their offices, in an office-based surgery facility. Personally, I favor a hospital-based surgery center for all surgeries requiring anesthesia. I have never performed rhinoplasty in an office-based facility. If you select a surgeon performing surgery in an office-based facility, at a minimum, you should be sure that this facility has passed a rigorous credentialing process.
The Surgical Team
There should be an anesthesia team, the surgeon, a scrub nurse, and a circulating nurse. In the recovery room, there is a recovery room team, which typically includes a doctor, nurses, and also nurse assistants.
Chapter 3: Your Consultation
What to Expect
An office consultation is an exchange of information. You and the surgeon are interviewing each other! Your job is to assess whether he is the right surgeon for you. His job is to decide whether he thinks you are a good candidate for surgery.
What should I bring to my first visit?
Come with some thoughts about what you would like changed about your nose. Come with a written list of questions. Be prepared to tell us your medical history, any past surgeries (including all prior nasal surgeries), current medications, drug allergies, and so forth.
The Surgeon’s Evaluation of You
Questions the surgeon has for you:
Medical history – most of this will have been filled out by you in the form, and will be reviewed by the doctor with you. I want to be sure you are healthy, that you are medically fit for surgery.
What you don’t like and why? This is the “thesis statement” – the reasons you want surgery. Of all the things you tell the doctor, this is the most important information.
An example in primary rhinoplasty: “Doctor, my nose is too big for my face. Also, my tip is bulbous, and I don’t like my hump. There are some other things, but these are my major concerns.”
An example in revision rhinoplasty: ” Doctor, too much was taken in my last rhinoplasty – from my bridge, and from my tip. My nose is twisted, my tip is pointy looking and unnatural. Also, my profile is uneven. Also, I can’t breathe through my nose.”
This should be your lead-off statement to the doctor! Everything else you discuss with him, he will have your goals foremost in his mind. This approach will surely allow you to get the most out of your consultation.
Some patients like the doctor to look at their nose and tell them what is wrong with it. It is fine to proceed this way, but just make sure that at some point, you tell the doctor what you don’t like, what you want addressed!
Do you have Reasonable expectations This is discussed above, and is an important part of the evaluation.
What are your specific questions or concerns regarding the surgery process? Everyone has certain things that are particularly on their mind. Write these down, and discuss them with your doctor. Common questions/concerns are logistical, relating to the type of anesthesia, what recovery will be like, etc…
The Physical Examination
Question:Can you provide an example of a specific patient and your analysis of their nose and what you did for them?
Answer: Shown below is a patient who came to me in hopes of improving the appearance of his nose because he felt it was too big for his face and because he had trouble breathing. My first impression of the nose was that it was, indeed, too big for his face. When I examined his nose from the side, I discovered that he had a large nasal hump and that his nose was overprojected (it stuck out too far from his face). On a positive note, the length of this patient’s nose is just right, neither too long nor too short, and, from this angle, the nostrils have a normal shape.
Though the patient is not interested in a chin implant, I did notice that his chin was a bit underdeveloped. In fact, that’s likely why he chooses to wear a goatee as it adds a bit more prominence to the chin and facial balance.


A very subtle twist to the nose was seen after careful examination of the front view, though the patient himself had never noticed it before. Though some twist may persist, we planned to make every effort to improve this. The front view also shows that the nasal tip is a little full, which can be enhanced with some conservative refinement of the nasal tip. Also determined at this time was that the patient’s skin was of medium thickness and that his nose was of normal width.


I then examined the nose from the base or bottom view which reiterated that this patient’s nose sticks out too far from his face. Again, we found that the nose was not too wide for his face, but that the tip was a little full or bulbous. By feeling, or palpating, the outside of the nose, I discovered that he has relatively short nasal bones and relatively long upper lateral cartilages, which comprise the nose’s middle portion. It is important that we know this in order to provide the cartilaginous ‘middle portion’ of the nose with some extra support.
Question:Can you describe how a surgeon analyzes a patient’s nose, and how it deviates from the ideal?
Answer: A surgeon will first consider the ‘first impression’ of the nose, such as whether it’s too big, twisted, has a large hump or has been over-operated on. Often times, this first impression is what bothers the patient as well. The surgeon will also find out from the patient exactly what it is that he or she dislikes about their nose.
Next, the surgeon will examine the nose from the front. He will make a note of whether the nose is straight or twisted, whether the nasal tip is asymmetric, bulbous or otherwise abnormal, and whether the nose is too wide, too narrow or normal. The surgeon will also examine the skin to determine its quality, whether it is thick, thin or medium.
The nose is also examined from the side. This will allow the surgeon to determine whether the nose is too short or too long and if the profile of the nose has a hump or is a ‘ski slope’. At this time, the tip of the nose is also examined so the surgeon can determine if it is overprojected or underprojected or just right. The surgeon will also see if there is too much nostril show present.
The nose is examined from all angles in order to provide important information about the nasal anatomy that is crucial to the planning of a successful surgery. In addition, the surgeon will feel the nose.
Question:Can you provide an example of a specific patient and your analysis of their nose and what you did for them?
Answer: Shown below is a patient who came to me in hopes of improving the appearance of his nose because he felt it was too big for his face and because he had trouble breathing. My first impression of the nose was that it was, indeed, too big for his face. When I examined his nose from the side, I discovered that he had a large nasal hump and that his nose was overprojected (it stuck out too far from his face). On a positive note, the length of this patient’s nose is just right, neither too long nor too short, and, from this angle, the nostrils have a normal shape.
Chapter 4
When to Schedule
You should find out from your surgeon how far in advance you need to book your surgery. You should pick a time that is convenient for you, when you will be able to take the time to recuperate, and you will have the help you need while you are recuperating. The most popular time for surgery seems to be the summer, especially August, and also the winter, especially December.
Meet with the Surgeon
Review the Plan , Sign Consent, and review Logistical Details
Dr. Becker will meet you again in the office prior to surgery to re-examine you, and to review the surgical plan, the computer imaging, and answer any additional questions. Written permission (“surgical consent form”) is reviewed and signed. (A copy of Dr. Becker’s consent form is provided here.) Any outstanding logistical details are addressed.
What Will you Tell People
Based on the experience of our patients, most are able to go back to work, or out in the public eye, after a week without people really noticing that they had surgery. We are conservative in the advice we give, so to our patients who want to be most sure of being “clandestine,” we advise that they should wait 10 days from the day of surgery.
Believe it or not, most people’s visual memory is such that they generally will not notice the difference – they will notice that you look better, but generally will not be able to pinpoint the difference.
But, in case someone notices the swelling, or a scar or some bruising in the early healing phase, or some other clue of nasal surgery, it can be helpful to decide what you will tell people. Our patients’ tell us that, if they don’t want to say that they had cosmetic surgery, the easiest thing to say is that you had to have some surgery to fix a breathing problem.
Schedule Medical Tests
Based on your age and medical history, your surgeon will advise medical tests, including possible blood work, electrocardiogram, chest X-ray or other. The purpose is to assess your health to be sure that you are healthy enough to have a 2 hour operation under anesthesia.
Fill Prescriptions
We will give you prescriptions for after surgery – a pain medicine, an antibiotic, and an anti-nausea medicine to use if needed immediately after surgery. Also, we sometimes give patients medication to help them sleep prior to surgery. You should fill all these medications before the day of surgery, so you will not have to do this after.
Buy OTC Items
Some useful items are Q-tips, gauze, hydrogen peroxide, and 4 bags of frozen peas!
Caregiver
It is nice to be pampered a little. You should make arrangements to have some down time. Someone must be with you for a period of time after surgery.
Plan for your Recovery
Do’s and Don’ts
Please read & familiarize yourself with these instructions both BEFORE & AFTER surgery. By following them carefully you will assist in obtaining the best possible result from your surgery. If questions arise, do not hesitate to communicate with me and discuss your questions at any time.
BEFORE SURGERY INSTRUCTIONS:
*You are having surgery at the Kennedy Surgical Center, 540 Egg Harbor Rd., located directly in front of our office.
* Call the Kennedy Surgical Center at 856-218-4900 on __________________________, between 1-3 pm to find out what time you must report for surgery. Please call us if you experience any difficulty.
* You are required to have someone drive you to and from the Surgical Center. If you are an out-of-town patient or if you are having trouble arranging a ride, we will be happy to help arrange transportation to and from the Surgical Center, as well as to and from our office.
* You must stop using any aspirin or aspirin related medication 2 weeks prior to surgery, as well as, 1 week post op. This includes Ibuprofen, Advil, Aleve, Motrin, Bayer etc., in any form (Cold & Sinus, Tension Relief, Migraine etc).
* You have been provided with prescriptions for after surgery. You should have these filled prior to surgery so that they will be ready for you at home after surgery.
* You will be scheduled for a morning surgery; therefore, you are to have nothing to eat or drink after midnight the night before your surgery.
* We have contacted your family doctor in order to let them know you will be having a surgical procedure, and to request medical clearance. CALL YOUR DOCTOR to arrange a pre-surgical appointment with them to facilitate medical clearance.
* Your first post operative visit is on _______________________ at ___________. Someone should drive you to this visit.
* Regarding any insurance-related surgery, we will call your insurance to verify your benefits and coverage. We will find out if any co-pay, deductible or referral is necessary. Your primary doctor will be notified if a referral is required. We will also contact you if there is anything you need to do or pay in advance of your surgery. Should you have any questions regarding your benefits and coverage, feel free to contact Donna at our office.
AFTER SURGERY INSTRUCTIONS:
Take this list to the hospital with you and begin observing these directions on the day of surgery.
- Do not blow nose until instructed. Wipe or dab nose gently with Kleenex if necessary.
- Change dressing under nose (if present) until drainage stops.
- The nasal cast will remain in place for approximately one week and will be removed in the office. Do not disturb it; keep it dry.
- Avoid foods that require prolonged chewing. Otherwise, your diet has no restrictions.
- Avoid extreme physical activity. Obtain more rest than you usually get and avoid exertion, including athletic activities & intercourse.
- Brush teeth gently with a soft toothbrush only. Avoid manipulation of upper lip to keep nose at rest.
- Avoid excess or prolonged telephone conversations and social activities for at least 10-14 days.
- You may wash your face – carefully avoid the dressing. Take tub baths until the dressings are removed.
- Avoid smiling, grinning, and excess facial movements for one week.
- Do not wash hair for one week unless you have someone do it for you. DO NOT GET NASAL DRESSINGS WET.
- Wear clothing that fastens in front or back for 1 wk. Avoid slipover sweaters, T-shirts and turtlenecks.
- Absolutely avoid sun or sun lamps for 6 weeks after surgery; heat may cause the nose to swell. Thereafter, use sunscreens.
- Don’t swim for one month, since injuries are common during swimming.
- Following removal of the dressing, the nose, eyes, and upper lip generally show some swelling & discoloration – this usually clears up in 2-3 weeks. In certain patients it may require 12-18 months for all swelling to completely subside.
- Take only medications prescribed by your doctor(s).
- Do not wear regular glasses or sunglasses which rest on the bridge of the nose for at least 4 weeks. We will instruct you in the method of taping the glasses to your forehead to avoid pressure on the nose.
- Contact lenses may be worn beginning 2-3 days after surgery.
- After the doctor removes your nasal cast, the skin of the nose may be cleansed with a mild soap or Vaseline Intensive Care Lotion. BE GENTLE. Makeup may be used as soon as the bandages are removed. To cover discoloration, you may use “ERASE” by Max Factor, “COVER AWAY” by Adrien Arpel, “ON YOUR MARK” by Kenneth, or other makeup as directed by our office.
- DON’T TAKE CHANCES! – If you are concerned about anything you consider significant, call me.
- When we remove your splint, your nose will be swollen and will remain so for several weeks. In fact, it takes at least one year for all swelling to subside.
The Night Before, The Day Before
What to Wear to the Surgery Center, and after
Wear clothing that fastens in front or back for 1 wk. Avoid slipover sweaters, T-shirts and turtlenecks
Homeopathic medications
Many patients ask about the use of the supplements Arnica and Bromelain, for use after surgery to reduce the early swelling and bruising. I have never urged my patients to take these, because in my hands, the early swelling and bruising reliably goes down in 5-6 days, by the time the nasal bandage comes off. I attribute this to healthy patients and careful surgical technique.
There is more or less bruising depending on many factors, including the type and extent of procedure, the age and overall health of the patient, whether the patient is asmoker, whether the patient bruises easily, and many others. I do not object to the use of these treatments; I just have found that in healthy patients, and with good surgical technique, their effect appears minimal.
However, because it appears that there are few if any known side effects, some patients choose to use these products, on the chance that it may speed their recovery process.
Arnica
In herbal medicine, Arnica usually refers to Arnica montana, a mountain plant used for relief of bruises.
One Arnica product that is widely used is SinEcch. SinEcch is said to speed healing after a planned trauma like plastic surgery. SinEcch is a set of 12 capsules on a blister card with the information about when to take each dose printed right on the card. The dosage regimen is custom designed to match the level of bruising and swelling which most patients experience in the most common plastic surgery procedures, facelift, rhinoplasty (nose surgery), blepharoplasty (eyelid surgery), liposuction, etc.
Pineapple extract – Bromelain
Bromelain is an anti-inflammatory formula containing the proteolytic enzyme from the stems of pineapples. Proteolytic enzymes are capable of dissolving proteins. It is most often used after sports injuries, to relive edema and after surgical procedures to help with swelling.
Arnika Forte is the only combination product of homeopathic Arnica Montana, Bromelain, grape seed extract, and Rutin in a capsule formulation. Grape seed extract and Rutin are products that are said to speed healing. You can find these products online; and we also do make this product available in our office.
Chapter 5
Arrive at the Surgery Center
We ask each patient to call the surgery center the day before surgery. They will tell you what time to arrive. When you arrive on the day of surgery, you will check in at the registration desk. You will be taken back to the pre-surgery area by one of the nurses. You will be taken to a private room, where you will be able to change into a surgical gown.
Meet the Surgeon
Dr. Becker will meet you in the pre-surgery area, to say hello, to review a final checklist of items (do you have any last-minute questions? Do you have your prescriptions filled? Etc…) He may see you before you have had the IV and met the anesthesiologist, or after.
Meet the Anesthesiologist
An anesthesiologist will meet with you, review your medical history, examine you, and discuss your anesthesia with you.
Placement of the IV
A nurse will place your IV. If you are afraid of needles, our skillful nurses take special measures to make you comfortable in this essential step.
Anesthesia
Sedation v. General
Dr. Becker performs rhinoplasty with the patient under general or sedation anesthesia. These days, he is finding that more patients seem to prefer general anesthesia, but either way is fine with Dr. Becker. Under sedation, your nose and surrounding areas will be numb and you will drift in and out of sleep. With general anesthesia, you will be asleep for the entire procedure.
Monitoring During Anesthesia: Regardless of the type of anesthesia used, you are carefully and thoroughly monitored before, during and after your surgery.
THE SURGERY
Question: What kind of advanced technology and modern techniques do you use to achieve faster healing and more precise surgery?
Answer: I have designed a number of specialty instruments for rhinoplasty. These instruments are smaller to allow me to perform more exact surgery.
For example, the “standard” osteotome (bone knife) for cutting the nasal bones is relatively large – too large in my opinion. We were able to measure the thickness of the nasal bones (only 2.5 to 3 mm) and have introduced a 2.5 mm and 3.0 mm guarded osteotome (manufactured by Microfrance), that we now use exclusively. We find that there is the least amount of trauma when these small instruments are used, and subjectively patients seem to have less bruising and heal faster.
In the operating room, I use the Becker/Toriumi Rhinoplasty Instrument Set, manufactured by Medtronic Corporation and especially designed for minimally traumatic rhinoplasty surgery.
The Bandage
A small nasal bandage is placed at the end of surgery, that you will wear for 5 or 6 days. An example is shown here.
Packing
Dr. Becker has not found packing necessary in any rhinoplasty patient. So, you can expect that you will not have nasal packing.
Recovery Room
After surgery, you will be taken by stretcher to the recovery room, where a team of nurses and the anesthesia team will monitor you and oversee your continued, rapid recovery from anesthesia.
Leaving the Surgery Center
When you have met all recovery room requirements, you will be allowed to leave the Surgery Center. You will need to have normal vital signs, be without significant pain or bleeding, be able to eat or drink something, and go to the bathroom. This recovery process usually takes about an hour.
Question: What kind of planning does Dr. Becker do for each rhinoplasty?
Answer: Careful pre-surgical planning is an important part of rhinoplasty. Dr. Becker typically “performs” each surgery at least 6 times:
- first (mentally) during the patient’s first office visit,
- again upon additional reflection,
- a third time after careful review of the preoperative photography,
- a fourth time just prior to the actual surgery,
- a fifth time is the ACTUAL surgery, and then
- the sixth (and more) times after the surgery as review, “post-surgery analysis.”
Chapter 6
Recovery at Home
Postoperative Instructions
Take only medications prescribed by your doctor(s).
Caring for you Nose
Do not blow nose until instructed. Wipe or dab nose gently with Kleenex if necessary.
Change dressing under nose (if present) until drainage stops.
The nasal cast will remain in place for approximately one week and will be removed in the office. Do not disturb it; keep it dry.
Brush teeth gently with a soft toothbrush only. Avoid manipulation of upper lip to keep nose at rest.
You may wash your face – carefully avoid the dressing. Take tub baths until the dressings are removed.
Do not wash hair for one week unless you have someone do it for you. DO NOT GET NASAL DRESSINGS WET.
Wear clothing that fastens in front or back for 1 wk. Avoid slipover sweaters, T-shirts and turtlenecks.
Sleeping on Your Back
Minimize Swelling and Bruising
Resuming Activities
Avoid excess or prolonged telephone conversations and social activities for at least 10-14 days.
Avoid smiling, grinning, and excess facial movements for one week.
Avoid extreme physical activity. Obtain more rest than you usually get and avoid exertion, including athletic activities & intercourse.
Food and Drink
Avoid foods that require prolonged chewing. Otherwise, your diet has no restrictions.
Avoid Sunglasses
Do not wear regular glasses or sunglasses which rest on the bridge of the nose for at least 4 weeks. We will instruct you in the method of taping the glasses to your forehead to avoid pressure on the nose.
Contact lenses may be worn beginning 2-3 days after surgery.
Avoid the Sun, Avoid Swimming
Absolutely avoid sun or sun lamps for 6 weeks after surgery; heat may cause the nose to swell. Thereafter, use sunscreens.
Don’t swim for one month, since injuries are common during swimming.
Pain Management
Take only medications prescribed by your doctor(s).
Side Effects after Surgery – Bruising, Swelling, Drainage, Stiffness, Depression
When we remove your splint, your will be swollen and will remain so for several weeks. In fact, it takes at least one year for all swelling to subside.
Following removal of the dressing, the nose, eyes, and upper lip generally show some swelling & discoloration – this usually clears up in 2-3 weeks. In certain patients it may require 12-18 months for all swelling to completely subside.
Complications
Early – Infection, Bleeding
Late – Cosmetic
When to Call Your Surgeon
DON’T TAKE CHANCES! – If you are concerned about anything you consider significant, call me.
Followup Appointments
Dr. Becker will typically see you the day after surgery, if needed, and 5-6 days after surgery to remove your bandage.
Getting Back to Normal
Following removal of the dressing, the nose, eyes, and upper lip generally show some swelling & discoloration – this usually clears up in 2-3 weeks. In certain patients it may require 12-18 months for all swelling to completely subside.
After the doctor removes your nasal cast, the skin of the nose may be cleansed with a mild soap or Vaseline Intensive Care Lotion. BE GENTLE. Makeup may be used as soon as the bandages are removed.
Chapter 7
Question: What kinds of complications can occur in rhinoplasty?
Answer: Complications in rhinoplasty may be categorized as functional (related to breathing) or aesthetic (related to appearance); there may be elements of both. Problems after rhinoplasty commonly are due to underresection (not enough taken off), overresection (too much taken off), and/or asymmetry. Also, sometimes abnormal scarring is a problem after rhinoplasty.
In general, it is easier to fix problems relating to under-resection, because they can be fixed by going back and “taking a little more.” Problems caused by overresection can be a little more complicated because material needs to be added, and technical factors arising from the need to add tissue must be considered. Asymmetries can usually be improved and at times can be completely fixed.
Question: What can I do before surgery to decrease the risk of complications?
Answer: See Choosing a Plastic Surgeon. Once you have chosen a surgeon, have a candid discussion with the surgeon regarding your goals and expectations of surgery. A discussion of the potential complications is critical, so that you understand the risks of a complication.
Despite the best efforts of a talented surgeon, a complication can still occur. Although most complications are relatively minor and correctable, more serious, debilitating, and uncorrectible complications do occur .
Question: Is there any way to be certain that I won’t have a complication?
Answer: NO. There is no way to be certain that a complication will not occur. For example, unanticipated technical problems can occur during surgery that can lead to a complication. Surgery is not an exact science, and results cannot always be anticipated. Despite careful pre-operative analysis and meticulous attention to surgical detail, unacceptable results may still occur.
No surgical procedure should be taken lightly; a slight but real risk is involved in all surgery. Fortunately, the overwhelming majority of plastic surgery results are highly satisfactory and pleasing when accompanied by careful presurgical planning, meticulous surgery, and full patient cooperation.
Question: What should I expect in the way of communication with my surgeon?
Answer: The rhinoplasty surgeon must take great care to minimize the incidence of both functional and cosmetic complications. Your surgeon should be willing to take the time to explain the steps they take to minimize the risks of complications.
It is essential that the surgeon knows what the patient wants, and that the patient knows what the surgeon is planning. With this in mind, Dr. Becker has a clear conversation with his patients on this subject. Also, we review Computer Imaging with most patients to improve communication, to make sure the patient and surgeon are “on the same page.”
With computer imaging, Dr. Becker shows the patient an imaging result that is the goal for surgery, and he wants to be sure that the patient agrees to the goal. The patient understands that this is not a guarantee, but that this is our shared goal.
Question: What kind of planning does the surgeon do for my surgery?
Answer: It has been said that a rhinoplasty surgeon should “perform” the surgery at least 6 times: first (mentally) during the patient’s first office visit, again upon additional reflection, a third time after careful review of the preoperative photography, a fourth time just prior to the actual surgery, a fifth time is the ACTUAL surgery, and then the sixth (and more) times after the surgery as review, “post-surgery analysis.”
The patient should try to pick a surgeon who seems to care about and take a special interest in this unique operation, and who has demonstrated skill in the operation.
Question: How can I be sure he is a careful and conservative surgeon?
Answer: It is difficult to know for sure. However, one should seek a surgeon who demonstrates a conservative approach to rhinoplasty, who avoids over-aggressive resection maneuvers, who focuses on maintaining structural support, who seeks a natural unoperated appearance.
Question: What can I do before surgery to decrease the risk of complications?
Answer: Choose your surgeon carefully. Once you have chosen a surgeon, have a candid discussion with the surgeon regarding your goals and expectations of surgery. A discussion of the potential complications is critical, so that you understands the risks of a complication. Although most complications are relatively minor and correctable, more serious, debilitating, and uncorrectable complications do occur. Your surgeon will give you instructions for before and after surgery, be sure to follow them.
Question: If the surgeon does everything discussed here, can I be certain that I won’t have a complication?
Answer: NO. Even if your surgeon does things well, a complication can occur. Just as an airplane can encounter unexpected turbulence, unanticipated problems can occur during surgery that can lead to a complication. Surgery is not an exact science, and results cannot always be anticipated. Despite careful pre-operative analysis and meticulous attention to surgical detail, unacceptable results may still occur.
Question: If I ask my surgeon what percentage of his rhinoplasties are perfect, what answer should I expect?
Answer: A good surgeon is highly self-critical of his work. One famous master rhinoplasty surgeon was asked, toward the end of a career in which he had performed many thousands of rhinoplasties, how many “perfect” rhinoplasties he had done. After some thoughtful reflection, he replied, “two.”
With this in mind, you can imagine that in many cases the surgeon may notice a relatively subtle abnormality that is amenable to correction, but the patient may not even notice it or may not be concerned by it.
For more detailed information, see the Appendix. Also, See Dr. Becker’s textbook chapter entitled Complications of Rhinoplasty
In Closing
The “ideal nose” is one that is harmonious with your other favorable facial features. Our perception of beauty helps define what makes an ideal shape for a female or male nose. There is also a bit of an artistic element to this, so the ideal cannot be boiled down to simple lines and numbers. However, artists and plastic surgeons alike have devised some guidelines or proportions that represent the aesthetic ideal. This was done by studying faces that are universally thought to be beautiful. (see Knowledge is Power). Artists have long made studies of beauty and aesthetic proportions and, today, facial plastic surgeons must similarly understand beauty in order to make changes that can enhance their patients’ beauty.
Human beings are social creatures by our very nature, and to me, the importance of actual beauty in human life is proven to me time and again by the responses from patients after a successful rhinoplasty. I hope that this book was helpful, as you explore the possibilities of rhinoplasty.
Sincerely,
Daniel G. Becker MD FACS