Question: Is there an ideal nose and what is it?
Answer: A nose that is considered ‘ideal’ is one which is harmonious with the other favorable facial features. Our perception of beauty helps define what makes an ideal shape for a female or male nose. There is also always a bit of an artistic element to this, thus the ideal cannot always be boiled down to simple lines and numbers alone. However, artists and plastic surgeons alike can devise some guidelines or proportions that represent the aesthetic ideal by studying beauty and faces that are universally thought to be beautiful. Artists have long made studies of beauty and aesthetic proportions and, today, facial plastic surgeons must similarly understand beauty in order to make changes that can enhance their patients’ beauty.
Of course, much to your relief no doubt, some lines, numbers and measurements do exist. Shown below are the lines and measurements that facial plastic surgeons use as a guideline to the aesthetic ideal as reprinted with permission from The Rhinoplasty Dissection Manual by Rhinoplasty Surgeon and Philadelphia ENT Doctor Daniel Becker and associate Dr. Toriumi.
Major surface reference points are shown in the first two figures below. These will help you to understand the subsequent material on this page.
SURFACE ANGLES, PLANES & MEASUREMENTS
The “ideal” face, as shown below, can be divided into equal horizontal thirds:
Facial thirds:
(Figure 1)
Upper third: trichion to glabella
Middle third: glabella to subnasale
Lower third: subnasale to menton.
The “ideal” face, as shown below, can also be divided into equal vertical fifths:
Horizontal fifths:
(Figure 2)
Five equally divided vertical segments of the face.
The face must be in a standard position for reproducibility of measurements for the angles that follow. Some of these angles may change if the patient’s head is tilted down or up. The standard facial position used by most facial plastic surgeons is defined by the Frankfurt plane.
Frankfort plane:
(Figure 3)
Plane defined by a line from the most superior point of auditory canal to most inferior point of infraorbital rim.
The naso-frontal angle is the angle formed where the nose and forehead meet. The nose can appear relatively short if an overly sharp naso-frontal angle divides the forehead from the nose, whereas the nose may appear longer with an overly shallow angle.
Nasofrontal angle:
(Figure 4)
Angle defined by glabella-to-nasion line intersecting with nasion- to-tip line. Normal 115-130 degrees (within this range, more obtuse angle more favorable in females, more acute in males).
Forward protrusion of the nasal tip from the face (like Pinocchio) is known as nasal projection. Listed here are two reliable measurements of nasal projection:
Nasal projection: (Figure 5)
Forward protrusion of nasal tip from face.
Goode’s method – A line drawn through the alar crease, perpendicular to the Frankfurt plane. The length of a horizontal line drawn from the nasal tip to the alar line (alar point-to-nasal tip line) divided by the length of the nasion-to-nasal tip line. Normal 0.55-0.60.
Crumley’s method – The nose with normal projection forms a “3-4-5 triangle.” ie., alar point-to-nasal tip line (3), alar point-to-nasion line (4), nasion-to-nasal tip line (5).
The nasofacial angle is one way of assessing the projection of the nose from the face. The nose is likely too far from the face if the nasofacial angle is large, or the opposite may be true if the nasofacial angle is too short. You can simply look at the nose in profile in order to get an impression about projection, but these measurements add ‘science’ to the art of facial analysis.
Nasofacial angle:
(Figure 6)
Angle defined by glabella-to-pogonion line intersecting with nasion-to-tip line. Normal 30-40 degrees. [PEARL: “Normal” projection with a 3-4-5 triangle described by Crumley (see above) gives a nasofacial angle of 36 degrees.]
The nose can often appear larger when set against a small chin. A surgeon may analyze the role that adjustments to the chin may play in achieving facial harmony by paying attention to the nasomental angle (in conjunction with other measurements).
Nasomental angle:
(Figure 7)
Angle defined by nasion-to-tip line intersecting with tip-to-pogonion line. Normal: 120-132 degrees.
The lips should also be assessed by the surgeon to see whether they are in proper relationship to other facial parts.
Relationship of lips
to nasomental line:
(Figure 8)
Upper lip 4mm behind, lower lip 2 mm behind line from nasaltip-to-menton.
One desirable feature is a sharp mentocervical angle.
Mentocervical angle:
(Figure 9)
Angle defined by glabella-to-pogonion line intersecting with menton-to-cervical point line.
An acute nasolabial angle can lead to a droopy nose, whereas an obtuse nasolabial angle can lead to a short or ‘uplifted’ appearance.
Nasolabial angle:
(Figure 10)
Angle defined by columellar point-to-subnasale line intercepting with subnasale-to-labrale superius line; normal 90-120 degrees (within this range, more obtuse angle more favorable in females, more acute in males).
Too much or too little ‘columellar show’ is, from the side, undesirable. As shown here, there are a total of nine possible configurations for the alar-columellar relationship as there are three possible configurations for the columella (normal, hanging, or retracted) and another three possible configurations for the nostril rim or ala (normal, hanging, or retracted). One of these nine configurations must be diagnosed by the surgeon.
Columellar show:
(Figure 11)
Alar-columellar relationship as noted on profile view, 2-4 mm of columellar show is “normal.”
Question: What are some of the characteristics of the ideal female nose and the ideal male nose?
Answer: This ideal, whether for a female or male patience, is simply a frame of reference or a goal and it must be modified to take into account the particular facial features of each patient.
Question:Can you describe how a surgeon analyzes a patient’s nose?
Answer: Is important to know that Nasal surgery does not change the character of your face, it makes it more balanced and it is important to have an experienced plastic surgeon or ENT specialist do your surgery. The surgeon will first consider the ‘first impression’ of the nose, such as whether it’s too big, twisted, has a large hump or has been over-operated on. Often times, this first impression is what bothers the patient as well. The surgeon will also find out from the patient exactly what it is that he or she dislikes about their nose.
Next, the surgeon will examine the nose from the front. He will make a note of whether the nose is straight or twisted, whether the nasal tip is asymmetric, bulbous or otherwise abnormal, and whether the nose is too wide, too narrow or normal. The surgeon will also examine the skin to determine its quality, whether it is thick, thin or medium.
A side view of the nose is also examined. This will allow the surgeon to determine whether the nose is too short or too long and if the profile of the nose has a hump or is a ‘ski slope’. At this time, the tip of the nose is also examined so the surgeon can determine if it is over-projected or under-projected or just right. The surgeon will also see if there is too much nostril show present.
The nose is examined from all angles in order to provide important information about the nasal anatomy that is crucial to the planning of a successful surgery. In addition, the surgeon will feel the nose.
Question: Can you provide an example of a specific patient and your analysis of their nose and what you did for them?
Answer: Shown below is a patient who came to me in hopes of improving the appearance of his nose because he felt it was too big for his face and because he had trouble breathing. My first impression of the nose was that it was, indeed, too big for his face. When I examined his nose from the side, I discovered that he had a large nasal hump and that his nose was over-projected (it stuck out too far from his face). On a positive note, the length of this patient’s nose is just right, neither too long nor too short, and, from this angle, the nostrils have a normal shape.
Though the patient is not interested in a chin implant, I did notice that his chin was a bit underdeveloped. In fact, that’s likely why he chooses to wear a goatee as it adds a bit more prominence to the chin and facial balance.


A very subtle twist to the nose was seen after careful examination of the front view, though the patient himself had never noticed it before. Though some twist may persist, we planned to make every effort to improve this. The front view also shows that the nasal tip is a little full, which can be enhanced with some conservative refinement of the nasal tip. Also determined at this time was that the patient’s skin was of medium thickness and that his nose was of normal width.


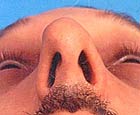
I then examined the nose from the base or bot tom view which reiterated that this patient’s nose sticks out too far from his face. Again, we found that the nose was not too wide for his face, but that the tip was a little full or bulbous. By feeling, or palpating, the outside of the nose, I discovered that he has relatively short nasal bones and relatively long upper lateral cartilages, which compromise the nose’s middle portion. It is important that we know this in order to provide the cartilaginous ‘middle portion’ of the nose with some extra support.