Although caudal septum treatment may appear as an auxiliary procedure to the novel surgeon,its inherent difficulties characterize this anatomical district as one of the most challengingin the nasal region. The nasal septum has a great influence on the global shape of the nose because it is strictly connected to all the bone and cartilage structures and is a paramount structure during growth.
The role of septal cartilage in providing architectural support and aesthetic influence to the nasal tip was emphasized by Metzembaum almost 80 years ago and even since 600 BC Sushruta Samhita (1-2) was indicating that with only external attempts in nasal reshaping, the residual septal deformity were going to limit the ultimate esthetic result, also worsening nasal function.
Therefore, “as goes the septum, so goes the nose”(Irving Goldman) is a well known expression of the pivotal role of this structure in conditioning aesthetics and function. In the very beginning, there have been many isolated reports focusing on surgical treatment of the quadrangular cartilage, but the most significant papers came from Ingals (3)Freer and Killian (4-5) with their description of the submucosal techniques, aimed for the correction of bone and cartilage deformities while maintaining the mucosa intact. Furthermore, Joseph (6)introduced the endonasal approach for rhinoplasty, and the combination of this with the transmucosal approach to the septum of Killian and Freer led to a period in which most septorhinoplasties were performed endonasallyin order to achieve a better nasal deformity correction.
Whether closed or open approach,nowadays there is a wide number of proceduressuitable to treatacaudal septal functional or esthetic abnormality, but every approach is effective only in a limited amount of cases, following the correct indications. This is due to the high number of anatomical structures involved.
Anatomy Of The Nasal Base
The surgical plan and the final outcomes can be mastered only after the comprehension of the functional anatomy of the discussed nasal area. As previously reported, the septum influences not only the function but also the shape of the nose, a concept that tends to be neglected even today (7). If not corrected, the nasal axis will stay deviated,negatively influencingthe aesthetics of the nasal base and of the whole nose.
The nose can be roughly divided into an upper,a middle and a lower third, and can present with deviation in one or in all three portions (8). This is not only the case of severe nasal traumas, but also a problem related to congenital deformities and can be visible also as secondary defect after primary rhinoplasties. Therefore, a deep knowledge of the surgical anatomy is mandatory in order to plana correct surgical schedule. Today there is a comprehensive description of the nasal anatomy, although the extent of the anatomic-pathological knowledge of septum deviation was poor until 100 years ago; the first systematic report dates back to the second half of 19th century with Theile (9).Even though the different caudal septum deformities will now be described and classified, the anatomy of the whole nasal septum and of the surrounding areaswill also be discussed in order to provide the surgeon with a grid suitable for the repositioning of the altered structures during treatment planning.
Composed primarily of the quadrangular cartilage, vomer (bone), and perpendicular plate of the ethmoid bone, the septum rests on the nasal spine and the nasal crest of the maxillary and palatine bones inferiorly in a “tongue and groove” fashion. The portion of the septum that develops into the perpendicular plate then ossifies during growth. It is remarkable that the inferior support structures (vomer and crest, Fig 1) origin from separate ossification centers and develop bilaterally from each side ofthe inferior septum and eventually mergingwith it.
The nasal cartilagineousseptum divides the nasal cavities, gives support to the nasal vault and provides support to the nasal mucosa which has a crucial functional role on each side, and influences the nasal airflow. Finally, it gives shape and support to the columella and to the nasal tip(10).Caudally, the attachments are to the medial crural footplatestrough the membranous septum and to the lower lateral cartilage by dense connective tissue at the domes.
Dorsally the cartilaginous septum joins the upper lateral cartilages, and has the critical attachment to the nasal bone at the rhinion. The perpendicular plate of the ethmoid attaches rostrally to the nasal bones, cribriform plate, and sphenoidal sinus. The vomer also fuses with the sphenoidal sinus rostrally (Fig 2).
Given the previously describedaesthetic and functional features, quadrangular cartilage resection should be avoidedwhenever possible. Its exteriorizationis preferable (7),preserving the structure in case of future need for nasal reconstruction.
Because of the embryological derivation of the bony and cartilaginous portions of the septum from unossified perpendicular plate, the septum is covered by a continuous mucosal layer of mucoperichondrium (cartilaginous portion) and mucoperiosteum (bony portion). Although the mucosa may appear continuous in this region, there is clinically a tight fibrous attachment between the mucoperichondrium and mucoperiosteum at the “tongue and groove” articulation of the inferior quadrangular cartilage with the maxillary crest. This can cause a difficultsub-perichondral dissection of the septum and detachment from the nasal crest of the maxillary bone during surgery.Therefore in order to detach the nasal septum from the palatine groove it is necessary to perform a very careful undermining because of the tight junction between the two layers where mucosal perforations, particularly in post traumatic, congenital, secondary nose surgery cases, may be possible.
The most anterior part of the nasal septum is the area where the middle cruras interact. In this regionthree caudal septal anglescan be analyzed: the anterior angle, which stays immediately under the dorsal depression of the nasal tip, the intermediate, under the domes on the most prominent part of the columella which shapes the lobule infratip, and the posterior which is positioned on the junction of the quadrangular cartilage with the nasal spine (on the nasal labial angle) (Fig 3 a-b).
Membranous septum lies between caudal septum and columella. There is a comprehensive study of (11), which demonstrates through cadaver dissection the existence of a unique andcontinuous anatomical layer, the nasal SMAS, consisting of thenasal muscles. These muscles are the transverse nasalis muscle,the procerus, and the compressor naris major and minor. As far asthe levator labii alaeque nasi and the dilator nasi muscles are concerned,the discussion is still open, and the main opinion is that thesemuscles connect the nasal SMAS to the facial SMAS. At the level of the internalnasal valve, SMAS seems to divide into a superficial layer anda deep layer.
Each layer can be divided into medial and lateralexpansion. The superficial layer of the nasal SMAS passes superficiallyover the LLC: laterally, it inserts into the skin of the alarmargins, and medially, it joins the depressor septi nasi muscleat the nasolabial angle. The deep layer of the nasal SMAS runs deep to the superficiallayer; laterally, it inserts into the internal nasal valve witha fatty component; medially, it passes immediately anteriorto the anterior septal angle, and it runs posterior to the interdomalligament of the alar cartilages. Thus, the interdomal ligamentseparates the deep and the superficial medial expansions ofthe nasal SMAS. From outside to inside we can get in contact with the vestibular skin together with subcutaneous areolar tissue.
The laxity of this area can easily show any residual distortion of the quadrangular cartilage through the described fasciallayers, as well as of the middle cruras.The orbicularis as well as the depressor nasi muscles can exert at some point a traction on these structures drooping or elongating the nose.
Skin thickness also can influence tip and nasal base asthetics and therefore caudal septum morphology. The quality of subcutaneous tissue as well as the number of sebaceous glandscan modify the columellar shape.
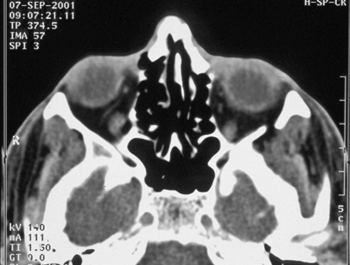
ANALYSIS: a series of pictures is collected(fig. 4a and b) in order to analyze the defect also basing our examination on the instrumental checks; a 3D CTscan of the upper airways to recognize even the smallest posterior defects should also be performed.
Classification of caudal septal deformities:
A series of 1600 rhinoplasties from 1993 to today were reviewed,recording the most frequent caudal septal deformities. These (see tab 1 and 2)have been summed up into the following groups:
–Overlong caudal nasal septum: a) congenital (see fig 5); b) grafts; c) wrong tongue in groove technique.
-Short caudal nasal septum: a) surgical overresection (see fig 6); b) congenital; c) nasal septal fracture(see fig 7).
-Deviation or asymmetry: a) post traumatic(see fig 8); b) congenital: c) post-surgical (see fig 9).
–various deformities: infections;scars (see fig 10); alar cartilage deformities; Drooping tip (post surgical in excessive resection of the nasal septum or in Le Fort I osteotomy).
Techniques
Aesthetics and function are strictly linked, and correction of a caudal deviation or a deformity of the septum must be done very precisely. The role of the caudal segment of septal cartilage in providing architectural support to the nasal tip was emphasized by Metzenbaumalmost 80 years ago. Any loss of caudal septal support would substantially affect the stability of nasal tip and thereby result in serious aesthetic as wellas functional problems(12).Aesthetically, maximum columellar show should not exceed 4 mm, which is the width of the typical medial crus (13). Excessive columellar show or a hanging columella may be caused by prominent medial crura, excessive membranous septal flaps, or a projecting caudal cartilaginous septum. Hanging columella needs to be distinguished from alar notching or retraction, which is often an undesired outcome of a previous rhinoplasty with overly aggressive resection of the lower lateral crura. This sometimes subtle deformity, if left uncorrected, can cripple an otherwise pleasing cosmetic result. Correction by other techniques often requires trimming of the caudal end of the cartilaginous septum, which, if overdone, can either foreshorten thenose or, paradoxically, lead to tip drop due to a decrease in medial crura attachments. Deviation of the caudal aspect of the nose may be related to a deviated caudal septum or asymmetries of the medial crura such as buckling. Correction of deviations in this area can be complex to achieve and difficult to maintain (14).
Anumber of techniques to treat those deformities are available. They can be:
PROBLEM: CAUDAL SEPTAL DEVIATION.
SOLUTION: SWINGING DOOR TECHNIQUE (8).
This technique allows the surgeon to disarticulate the quadrangular cartilage from the bony septal components and from the maxillary crest, preserving the keystone area.
By doing two mucoperichondral flaps, a retrograde dissection is performed,followed by a resection, if excessive,of the septal caudal segment and by the replacement of the nasal septum into the midline, stabilizing it during healing with 4-0 PDS sutures.
There are other manouvers that can be associated, such as thinning the caudal septum in a vertical plane, or crossbar septal grafts to be included in a combined surgical plan. Doing this technique neither scoring techniques nor the swinging door after excessive weakened septum in secondary cases should be associated.
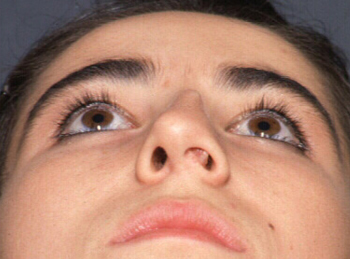
CLINICAL CASE: Patient affected by a severe caudal septal deviation and nasal hump in a crooked nose classical deformity. The case has been corrected through a delivery approach and a swinging door technique and caudal septal resection (see figures).
PROBLEM: SEVERE ANTERIOR SEPTAL DEVIATIONS, LOSS OF ANTERIOR SEPTAL CARTILAGE WITH POOR TIP SUPPORT.
SOLUTION: CAUDAL EXTENSION GRAFT:
The caudal extension graft is a cartilage graft that overlaps the dorsal or the caudal margin of the nasal septum and is sutured between the triangular cartilages or the medial crura to stabilize the nasal base and set tip projection and appropriate alar/columellar relationship. A minimum of two sutures should be applied to fix the caudal extension graft to the septum. The caudal margin of the extension graft should lie in the midline. To determine the position of the nasal tip and thenasolabial anglethe caudal extension graft is fixed posteriorly, and by doing this it will act to open the nasolabialangle. If the caudal extension graft is moved alongthe anterior margin, it will tend to counter-rotate thenasal tip. The caudal extension graft is also ideal for thecorrection of the retracted columella.
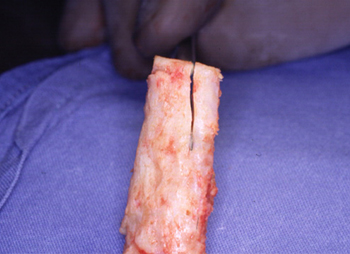
To prepare it,costal cartilagecan be harvestedor posterior septal cartilage extended columellar strut fixed to the periosteum around the nasal spine.The first, and most preferable, choice is autogenous septal cartilage, followed by autogenous conchal cartilage, and then by irradiated costal cartilage homograft. The dimensions of the graft depend mainly on the size of the missing caudal segment and the aesthetic goals of the operation. The length (antero-posterior dimension) of the graft is determined by the amount of tip projection needed; the width (cephalo-caudal dimension) ranges from 7 to 13 mm, depending on the extent of caudal septum deficiency, and the thickness of the graft ranges from 2 to 4 mm for autogenous grafts and from 3 to 6 mm for irradiated cartilage homografts. The mucoperiostium is easily elevated off the maxillary crest, and the flap elevation is continued upward to expose the ventral part of the septal cartilage that is attached to the maxillary crest. This is the best part to use for a CSR graft as it is the thickest part of septal cartilage and is usually found intact, even in revision cases with near-total absence of septal cartilage (12).
In case of underprojected nasaltip with acute nasolabial angle the medial crura and the nasal base are advanced on the stable strut to increase tip projectionand open the nasolabial angle. The extended columellar strut isusually fixed tothe periosteum about the nasal spine.
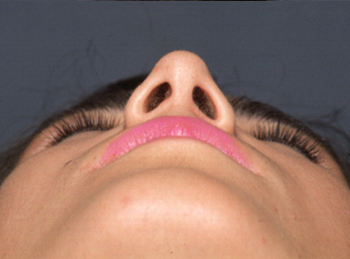
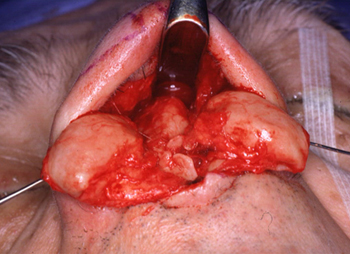
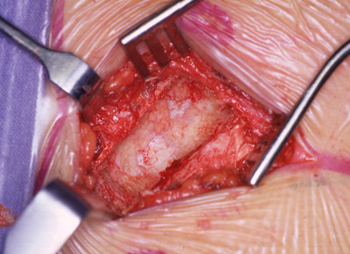
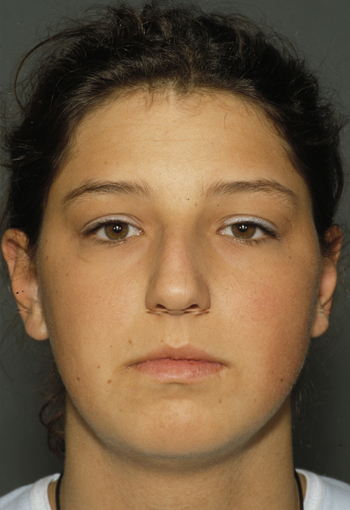
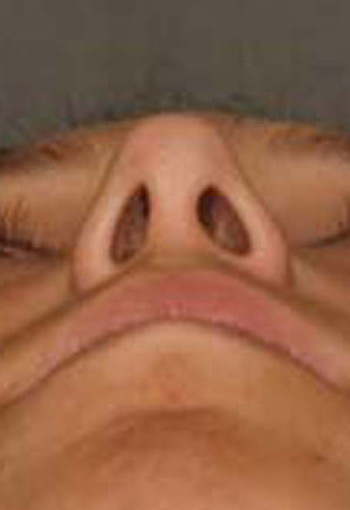
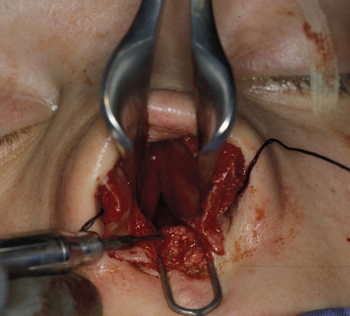
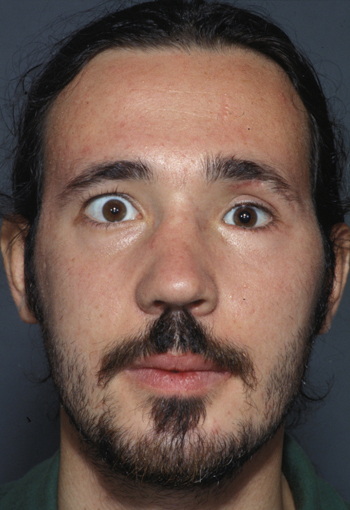
CLINICAL CASE: Patient affected by a severe caudal septal defect and dependent tip deformity with thick oily skin. The case has been corrected through an open approach , rib cartilage harvesting and caudal septal repositioning (see figures).
PROBLEM: SEVERE DEVIATION OF THE NASAL SEPTUM.
SOLUTION: SEPTAL ESTERIORIZATION (7):
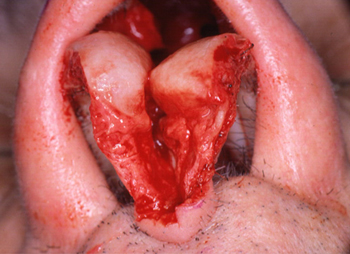
When the nasal septum heals in dislocation, the sharp angles or the concomitant nasal midline deviation are very difficult to be corrected. This is the case of cleft lip deformity, nasal trauma or secondary rhinoplasty. In this case extracorporeal septoplasty is one of the best options we have to solve the problem. After positioning topic Codman sponges with local anesthesia (naropine 7,5 mg ml with epinephrine 1:100.000) subperichondral injections of 1,8 ml are performed.The open approach was used in almost all of our cases, but it is possible to use the closed approach through a right sided hemitransfixed incision.
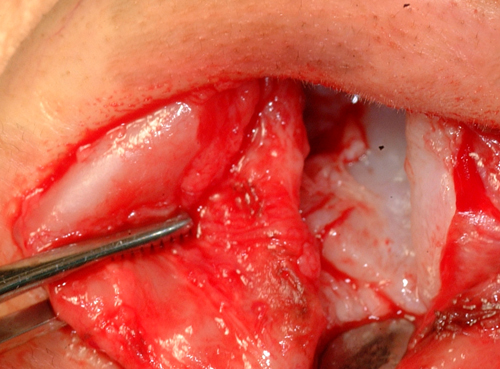
After the columellar access, the anterior angle of the nasal septum is exposed and the subperichondral dissection is then performed on the concave side of the septum continuing on the upper junction of the upper laterals. In this area we thereafter excise the hump, if necessary, or we completely free the nasal septum from the other bony and cartilagineous structures. Bony septum must be fractured with a 5mm chisel and the septal footplate is then detached.
At this moment the septum is exteriorized, then the excess cartilage is resected and cartilagineous scoring incisions are made. The septum can then be straightened suturing it to the perpendicular plate, a PDS foil or spreaders.
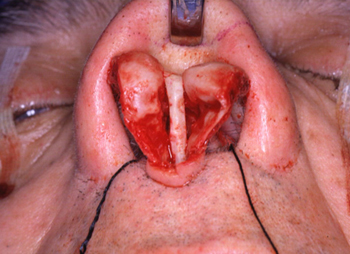
The septum gets finally replanted and fixed to the upper laterals with PDS 5-0 and U-shaped sutures. We then make a hole on the anterior nasal spine is subsequently performed and used as a supplementary fixation.A transeptal suture with vicryl rapid 4-0 is then performed, preventing dead space formation.
Gubisch (7), which is probably the most experienced surgeon on this technique, reports better results only with the following tips: infiltration with naropine, open approach, motor drill to smooth the septal surface, pds foil (only in cases of intact mucosa), precise reinsertion and stabilization with PDS sutures, dorsal coverage with fascia to reduce irregularities.
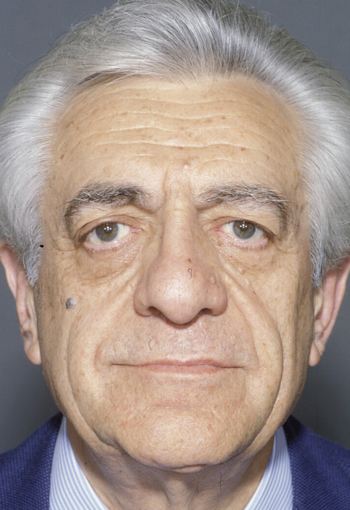
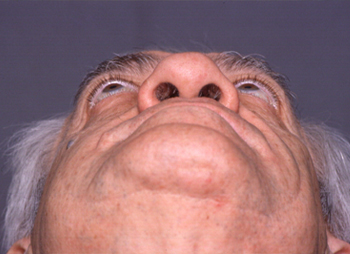
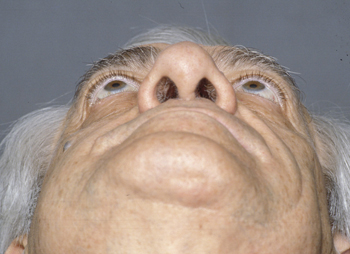
CLINICAL CASE: Patient affected by a severe caudal septal c shaped deformity and nasal hump with thick oily skin. The case has been corrected by W. Gubish together with us dring Rhinpplasty 2000 course organized with Eugene Tardy Jr. through an open approach, septal reshaping and repositioning (see figures).
PROBLEM: OVERRESECTED NASAL SEPTUM, SECONDARY SEPTAL LOSS DUE TO SEVERE TRAUMA OR CONGENITAL MALFORMATION.
SOLUTION: RECONSTRUCTION OF THE NASAL CAUDAL SEPTUM.
Most of the modern techniques for tip repositioning and caudal septal correction avoid excising caudal septal cartilage in order to maintain its vital role in supporting the nasal tip (15-16)Its shortening can derive from techniques involving caudal septal resections mainly to achieve superior tip rotation, to shorten the nose, or to correct complex caudal septal deviations. Also infections or Trauma or congenital malformations can cause this defect. Caudal septal deficiency is usually associated with variable degrees of premaxillary bone loss due to an underdeveloped, resected, or partially resorbed anterior nasal spine.
The caudal septum must be flat and flexible as all the external segment of the quadrangular cartilage (external to the skull). We can reconstruct it in several ways:rib cartilage for severe defective zones, ear cartilage for smaller defects, but it needs to be straightened with a PDS foil, irradiated cartilage, or PDS foil and Mersilene mesh (16).
This technique must be done with a transcolumellar incision and the most difficult step is the skin to skinor mucosa to mucosa dissection since there is no more cartilage in between. This is really an important step since as far as we reach the residual quadrangular cartilage, we must re-approximate the mucosal flaps to the inserted material, which is fixed with PDS 5-0, and to the native nasal septum. Nolst Trenite’ (17) suggests to graft a big piece (3X4), thinner than 1 mm to avoid widening of the nasal septum, easily attached to the cartilage and flexible.
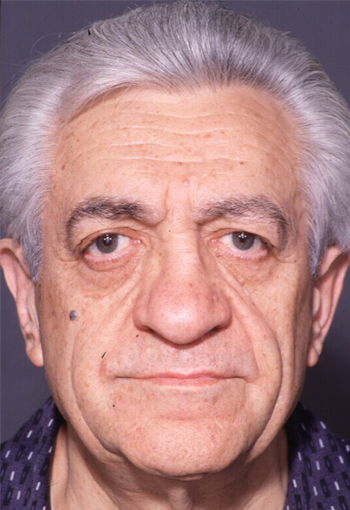
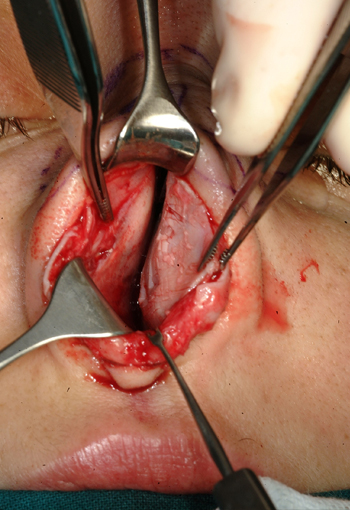
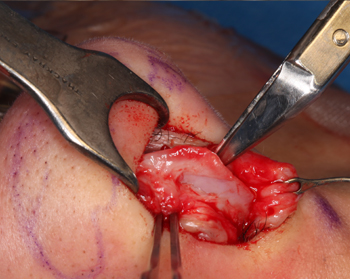
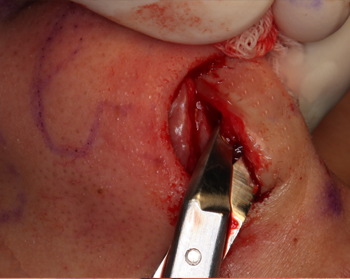
CLINICAL CASE: Patient affected by a severe midfacial trauma associated to a caudal septal fracture and nasal dorsum defect. The case has been corrected through an open approach, rib cartilage septal rebuilding and repositioning (see figures).
PROBLEM: CAUDAL SEPTUM DEVIATION, MEDIAL CRURA ASYMMETRY.
SOLUTION: INTERLOCKED GRAFTS, SEPTAL CROSSBAR TECHNIQUE,CARTILAGINEOUS SUTURES.
In any rhinoplasty procedure, a strong tip support is essentialto maintain the achieved degree of nasal tip projection and rotation; in other words, the long-term result of any tip-modifying technique will depend mainly on the amount of tip support available. One of the major challenges in rhinoplasty is to provide adequate tip support in cases in which the caudal septum was previously excised or is congenitally deficient.
When there is an intermediate nasal septal deviation, a single-interlocked graft inserted by 2 through-and through serial sections of the quadrangular cartilage (applied over the convex side previously scored on the concave side) facilitates adjustment of the distal septum intraoperatively. The strip of cartilage of the desired height and width acts as a spring graft and may be placed at the desired height of the caudal septal area to exactly counteract the eventual tendency of the most deviated area to warp over time. (18)
The oblique septal crossbar has inherent advantages over existing techniques for selected septal deformities. The anterior septal angle is preserved, and extracorporeal septoplasty may be avoided. Maintaining an intact L-strut retains the structural integrity of the nasal dorsum and tip. Furthermore, the crossbar resists the bowing of the dorsal septum that may otherwise occur with submucous resection. Because the crossbar is nearly perpendicular to the dorsum, it effectively withstands scar contracture. While the oblique septal crossbar graft offers many potential advantages, several caveats also warrant consideration. A wide graft may also widen the tip lobule in an asymmetrical fashion, particularly if it is placed medially to the intermediate crus of the lower lateral cartilage. In such cases, the dorsal end of the graft may be repositioned or sutures may be used to tighten the nasal tip. Because this graft is not in direct contact with the skin–soft-tissue envelope, untoward effects on the appearance of the external nose are unlikely. Also, if the crossbar is made out of cartilage with little rigidity, it may not confer the intended strength to the nasal dorsum. Adequate graft strength can be obtained for most patients with a cartilage of 2-mm thickness (the perpendicular plate may also be used). If the crossbar graft is too thick, it could create nasal obstruction. This concern can be mitigated by placing the dorsal end of the oblique septal crossbar graft along the concave side of a deviated dorsal strut. The narrower end of the graft may be placed along the dorsum to reduce the bulk of the graft-dorsum construct(19-20).
It was recently suggested by (21)that there are six different types of septal deviations, each one requiring a specific correction to achieve a satisfying outcome. They used extramucosal stents to correct the problems. In addition, the appealing alternative techniques of laser-assisted and endoscopic septoplasties were described.
Rubin(22) reported acceptable results in septal cartilage alienation bymorselization in a case series, but mentioned that there was stiffnessdiminution and a high grade of fibrosis that would make a second operation difficult to perform.The most frequently used techniques to straighten a curved cartilage are morselization and incisions of the entire cartilage thickness. Other authors extirpate a cartilage fragment or use complete repositioning of the cartilage septum anterior zone or use a combination of techniques Guiding sutures are placed on the anterior septal fragment—one at the top, entering through the nasal dorsum at the level of the cephalic edge of the lobular cartilage, and the other at the bottom, through the middle crura. By pulling the guiding sutures, the cartilage fragment is aligned to therest of the septum and placed into the receivingbag. Septo-columellar sutures are then insertedinto the septal mucosa, achieving thedesired fixed position and alignment.The modified mattress suture technique wascarried out as follows. Once the septum is dissected,partial-thickness incisions are made atthe point of maximum deflection on the concaveside, in a dorso-ventral direction, diminishingthe cartilaginous surface tension. The antero-caudal edge of the septumis fixed to the pre-spinal fibers with 4-0nylon suture using a figure-of-eight stitch. Themodified mattress stitch begins from the samesuture on the convex side, crossing over theseptal cartilage to the concave side, 5 mm beforethe relaxed incision zone, to do the samewith the posterior septal fragment. Both extremesare gently pulled until the cartilage isaligned and the knot is completed (23).
Regardless of the technique used to straighten the nasal septum, its reorientation can not prescind from its detachment from all the other structures and its subsequent reattachment to the nasal spine, the upper laterals and the alar cartilages.All these cartilages must be also reshaped to the new projected nasal structure. Therefore PDS 5-0 is used for the repositioning of the medial crura and give support to the tip fixing them to the nasal septum, or grafting a columellar strut, or with a tongue in groove technique. The same is for the dome reshaping and reunion, and lastly for reattaching the upper laterals to the nasal septum with or withoutspreader grafts.
CLINICAL CASE: Patient affected by a secondary deformity due to nasal trauma associated to a caudal septal fracture and nasal dorsum defect. The case has been corrected through an open approach, crossed septal incisions and repositioning (see figures).
PROBLEM: OVERLY LONG MIDLINE CAUDAL SEPTUM, POOR TIP SUPPORT, CONTROL OF NASAL TIP ROTATION AND PROJECTION.
SOLUTION: TONGUE IN GROOVE.
Patients who have an overly long midline caudal septum are good candidates for setting back the medial crura on the caudal septum. This technique is typically used in patients who would otherwise require trimming of the caudal margin of the nasal septum. In this case, the excessively long caudal septum is suture-fixated between the medial (24) crura in a tongue-in-groove fashion, and the redundant caudal septum is used to support the nasal tip. After dissecting between the medial crura, the caudal septum is identified. Then bilateral mucoperichondrial flaps are elevated, and redundant septal mucosa is moved cephalically, eliminating the need to trim septal mucosa after repositioning the nasal tip. The medial crura are repositioned on the caudal septum and then sutured to the septal cartilage with a 5-0 chromic mattress suture. If the tipposition, rotation, and alar/columellar relationship is appropriate, a 5-0 PDS suture is placed from the inner surface of both medial crura to the caudal septum. After the tip position is set and all septal work is completed, a running 5-0 plain gut suture on a straight septal needle is used to quilt the septal mucosa and redistribute the septal mucosa along the nasal septum.There are occasions when an under-projected nasal tip can be advanced anteriorly on the caudal septum to increase tip projection. When using this technique, it is critical to avoid creating aretracted columella, foreshortened nose, or over-rotated nasal tip lobule.
A full transfixion incision is created and the mucoperichondrium is elevated from the septum bilaterally in a posterior direction for at least 4mm to expose both sides of the caudal end of the cartilaginousSeptum. If septal deviations are present, the elevation of the mucoperichondrial flap is continued back to the bony cartilaginous junction on one or both sides. The deviated portion of the cartilaginous septum is then incised with the Cottle elevator, and the contralateral mucoperichondrial flap is elevated in the area overlying the section of cartilage to be removed. Efforts are made to preserve at least a 1-cm strut of dorsal and caudal cartilaginous septum to maintain nasal support. Any bony septal deviations are removed with the Becker scissors and polyp forceps. Nasal crest deviations are removed using the curved chisel and mallet after the laterally overlying mucosa has been elevated. A portion of the removed cartilage is crushed, replaced between the mucoperichondrial flaps, and secured in this position with a series of 4-0 chromic mattress sutures.
Bilateral membranous septum excision is almost always necessaryto remove excess tissue resulting from the TIG placement.Each side of the nose should be evaluated separatelyto determine the amount of mucous membraneexcision The membrane excision should take place posteriorto the transfixion incision. The created groove may vary in depth along the lengthof the medial crura. To allow a greater degree of upwardnasal tip rotation, the depth of the medial crural pocket andthe amount of denuded corresponding caudal septum shouldbe greatest at the dorsal or anterior aspect. On the otherhand, to inferiorly rotate the nasal tip or to correct excesscolumellar show in the posterior region, the deepest portionof the pocket and greatest corresponding advancementshould be placed posteriorly. The caudal septum maybe variably trimmed when necessary, depending on the correctionrequired. Furthermore, once the caudal septum isplaced into the groove, the medial crura may be advancedanteriorly toward the dome cartilages and fixed with suturesin this position to increase and help maintain nasaltip projection. Placement of the septal-columellar sutures and closure ofthe transfixion incision may be delayed until after other tiptechniques are performed. When caudal deviation is causedby asymmetry of the medial crura, an open approach is typicallyused to correct the asymmetry before final TIG positioningand placement of the septal columellar sutures. Incases of caudal septal deviation, the deviation should becorrected by freeing up the caudal attachments of the septumat the crest and spine. Once the septum has beenstraightened, placement of the caudal aspect between themedial crura adds further support to help maintain the septumin the straightened position.
CLINICAL CASE: Patient affected by a severe caudal septal deviation. The case has been corrected through transcartilagineous approach, septal repositioning (see figures).
PROBLEM: OVERLY LONG MIDLINE CAUDAL SEPTUM, POOR TIP SUPPORT, CONTROL OF NASAL TIP ROTATION AND PROJECTION.
SOLUTION: NASAL SPINE OSTEOTOMY
In patients with mildcaudal excess, conservative repositioning of the columella-labialjunction is achieved with partial reduction of theovergrown skeletal anatomy. This often involves only amodest trim of the caudal septum at the posterior septalangle. In patients with intermediate caudal excess, moreaggressive resection of the caudal septum and/or reductionof the nasal spine (with or without partial reductionof the premaxilla) may be needed to achieve sufficientretrodisplacement of the columella-labial junction.Alternatively, the tongue-in-groove setback technique can be used to achieve retro-displacement of the columella-labialjunction without aggressive skeletal resection. Sincethe tongue-in-groove setback technique minimizes tissueexcision and conserves skeletal support, I often favorthis approach in patients who have previously undergone septoplasty or who have weak or fractured septalcartilage. However, in patients with extreme caudal excess,aggressive skeletal reduction is mandatory, since thetongue-in-groove setback technique alone cannot providesatisfactory retrodisplacement of the protruding nasalbasemany prominent surgeons have cautioned againsttotal excision of the nasal spine due to the potential riskfor columellar retraction and/or compromised nasal-tipsupport (25) warned that the entire nasal spine should”never” be removed to prevent a “recessed nasolabialangle.” Instead, he advised judicious trimming of the caudalseptum and only “partial” trimming of the nasal spinein patients with a “crowded upper lip.” Peck also recommendedperforming ancillary soft-tissue proceduresof the upper lip, such as frenulectomy and V-Y mucosaladvancement, to reduce the overly prominent nasolabialangle. Like Peck, Sheen and Sheen advocated only”cautious” reduction of the nasal spine, arguing that nasalspine reduction is necessary in “less that 1% of cases.” Anderson and Ries also cautioned against complete nasalspine resection to prevent compromise of “its septalsupportive function.”In a more recent analysis of nasal-base aesthetics, Friedman and coworkers proposed a systematic classificationscheme for nasolabial angle deformities in patients undergoing cosmetic rhinoplasty. Later, Honrado and Pearlman published a 10-year clinicalfollow-up of this same classification system. In bothreports, profile deformities of the nasal base were subdividedinto distinct morphologic characteristics on thebasis of caudal septal length, nasal spine protrusion,and fullness of the nasolabial angle (ie, the presence of apushing philtrum). This classification scheme representsthe first formal attempt to systematically categorizethe structure of caudal excess in order to facilitatepreoperative patient analysis. In addition to a standardized classification system for caudal overgrowth, thearticle also describes various surgical treatment options,including reduction of the caudal septum, nasal spine,or both. Although the authors note the historical tabooassociated with nasal spine reduction, which likelyoriginated from the perceived risk of columellar retraction,their 10-year clinical experience with nasal spin excision was uniformly favorable. Moreover, Friedman and coworkers estimated that some degree of nasalspine reduction was essential in approximately 20% ofpatients with caudal overgrowth.
CLINICAL CASE: Patient affected by a caudal septal columellar deviation and nasal dorsum defect. The case has been corrected through an open approach, rib cartilage septal rebuilding and repositioning (see figures).
Conclusions:
Success in rhinoplasty is partly related to thesurgeon’s ability to control nasal tip projection. Excessive excision of the caudal margin of the septum can result in foreshortening of the nose and postoperative loss of tip projection. The incidence of many of these complications may vary from patient to patient. It is the responsibility of the surgeon to identify the predisposing anatomic variants and make necessary adjustments in surgical technique to avoid complications.(24)It isalso very important to control and obtain a straight midline and create harmonic brow-tip esthetic lines.
The following steps are mandatory to obtain a good result:
- Perform a proper analysis: clinical, instrumental (3D TC of the upper airways) and with accurate observation of the pictures.
- Complete mobilization of the nasal septum and of the surrounding structures.
- Correction of the nasal septum anatomical irregularities and also of the interrelated cartilagineous and bone structures.
- Stabilization of the reconstructed anatomy.
Bibliography
1. Johnson CM Jr: The deviated nose-Its correction. Laryngoscope 87:1680-1684,1977.
2. Snell D: History of external rhinoplasty. J Otolaryngol7:231, 1978.
3. Ingals E.F.: Deflections of the nasal septum. Arch Otolaryngol 1882;3;291-299.
4. Freer O.: Deflections of the nasal septum. Ann Otol213,1905.
5. Killian G: The submucous window resection of the nasal septum. Ann Otol363,1905.
6. Joseph J: Die Korrektur der Schiefnase. Deutsche Medizinische Wochenschrift 3:2035-2040, 1934.
7. Gubisch W.: Twenty-five Years Experience with Extracorporeal Septoplasty. Facial pLastic Surgery Vol:22 230-239 November 2006.
8. Pastorek NJ, Becker DG.: Treating the caudal septal deflection.Arch Facial Plast Surg. 2000 Jul-Sep;2(3):217-20.
9. Theile F.W.: Beitrage zur angiologie und Osteologie des Menschen. 5. Die Nasenscheidevand. Ztsch fur rationelle Medizin, II. Folge 1855;6:242-244.
10. E. Tardy Jr Rhinoplasty The Art and The Science, W.B. Saunders, Chicago 1999.
11. Saban Y, Andretto Amodeo C, Hammou JC, Polselli R.An anatomical study of the nasal superficial musculoaponeurotic system: surgical applications in rhinoplasty.Arch Facial Plast Surg. 2008 Mar-Apr;10(2):109-15.
12.Foda HM. The caudal septum replacement graft.Arch Facial Plast Surg. 2008 May-Jun;10(3):152-7.
13. Kridel RWH, Lunde K. Nasal septal reconstruction: review and update. Facial Plast
Surg Clin North Am. 1999;7(1):105-113.
14. Kridel RW, Ashoori F, Liu ES, Hart CG. Long-term use and follow-up of irradiated homologous costal cartilage grafts in the nose.Arch Facial Plast Surg. 2009 Nov-Dec;11(6):378-94.
15. Adamson PA, Tropper GJ, McGraw BL. The hanging columella.J Otolaryngol.1990;19(5):319-323.
16. Foda HMT, Kridel RWH. Lateral crural steal and lateral crural overlay: an objectiveevaluation. Arch Otolaryngol Head Neck Surg. 1999;125(12):1365-1370.
17. Nolst Trenite GJ. Grafts in nasal surgery. In: Rhinoplasty: A Practical Guide toFunctional and Aesthetic Surgery of the Nose. Amsterdam, the Netherlands: KuglerPublications; 1993:45-56.
18.Giacomini P, Lanciani R, Di Girolamo S, Ferraro S, Ottaviani F.: Caudal septal deviation correction by interlocked graft technique.Ann Plast Surg. 2010 Sep;65(3):280-4.
19. Kridel RW, Soliemanzadeh P.Tip grafts in revision rhinoplasty.Facial Plast Surg Clin North Am. 2006 Nov;14(4):331-41,
20. Boccieri A. Evolution of the septal crossbar graft technique. Facial Plast Surg. 2006;22(4):255-265.
21.Mowlavi A, Masouem S, Kalkanis J, Guyuron B.Septal cartilage defined: implications for nasal dynamics and rhinoplasty.Plast Reconstr Surg. 2006 Jun;117(7):2171-4.
22. Rubin FF.: Permanent change in shape of cartilage by morselization.Arch Otolaryngol. 1969 Apr;89(4):602-8.
23. Ponsky D, Eshraghi Y, Guyuron B.The frequency of surgical maneuvers during open rhinoplasty.Plast Reconstr Surg. 2010 Jul;126(1):240-4.
24. D.M. Toriumi / Facial Plast Surg Clin N Am 13 (2005) 93–113.
25. Peck GC.:Secondary rhinoplasty.Clin Plast Surg. 1988 Jan;15(1):29-41.26.
Figure Legends
Clinical Case Swinging Door






Clinical Case Caudal Extension




Clinical Case Septal Exteriorization
This case have been done by and together with Wolfgang Gubish during a Rhinoplasty Course in Verona








Clinical Case Septal Reconstruction






Clinical Case Crossed Incisions










Clinical Case Tongue In Groove









Clinical Case Nasal Spine Osteotomy






Tab 1: Basal view: nasal tip secondary defects
| Skin defects | 1.5% |
| Double domes | 1.86% |
| Left asymmetry | 5.14% |
| Right asymmety | 8.87% |
| Nasal spine deviation | 3.5% |
Tab 2: Basal view: nasal tip secondary defects
| Overexposed | 8.99% |
| Underexposed | 8.99% |
| Drooping tip | 0.46% |
| Flat columella | 2.11% |
| Absent nasal spine | 2.5% |