Introduction
The nose is a complex structure comprised of a bony-cartilaginous scaffold encased in a soft tissue envelope. These different tissue consistencies work intimately to develop the structure of the nose. In rhinoplasty, establishing form and function of this complex structure often requires grafting to the existing foundation. Conventionally, septorhinoplasty techniques often employ autogenous cartilaginous grafts including septal, auricular, or costal grafts. Septal cartilage is desirable for several factors: its wide and flat structure, its strength, its decreased tendency for warping, and its accessibility in the surgical field. [1] However, in complex structural and reconstructive rhinoplasty where significant grafting is required or in patients with diminutive cartilaginous nasal septum, the amount of the septal cartilage graft may be insufficient. By utilizing the bony septum, the amount of grafting material from the site can be enhanced. In addition, perpendicular plate of the ethmoid bone has several excellent qualities: its strength, thin profile, and flat contour make it a useful grafting material. This chapter describes our technique utilizing the septal osteocartilaginous graft in rhinoplasty to maximize the utility of this versatile autogenous graft.
Septal Anatomy
The nasal septum is composed of the quadrangular cartilage, the perpendicular plate of the ethmoid bone, the vomer, the maxillary crest, and the anterior nasal spine. The bony and cartilaginous septum is covered by mucosa on both sides. When harvesting septal grafts, the mucosa has to be carefully elevated off of the bony and cartilage septum and kept intact to prevent post-operative septal perforation.
Surgical Technique
The harvest of the septal graft can be done through both an endonasal or open approach. The mucoperichondral flaps are raised in standard fashion on both sides with particular attention to elevate the flaps into the bony septum posteriorly.
The planned harvest site is then outlined with care taken to leave at least 1.5cm dorsal and caudal strut to preserve the integrity of the dorsal and tip support. The authors prefer a 15 blade to make the dorsal, inferior, and caudal cartilaginous incisions. The dorsal cartilaginous incision is then completed with Fomon dorsal nasal scissors. The dorsal and inferior bony septal cuts were then made with Gorney nasal shears scissors. Care must be taken when manipulating the dorsal aspect of the septum not to disrupt the keystone area or the cribriform to avoid saddle nose deformity and/or skull base fracture with cerebrospinal fluid leak [2], respectively. The bony posterior incision is then completed with a Cottle elevator or a 2mm curved osteotome. There is usually a thin bony area past the bony cartilaginous junction and just before the thicker sphenoid crest and rostrum. Once all the cuts are completed the osteocartilaginous septal graft can be removed from the nose and saved for later use. (Figure 1). The harvested graft would include portions of the quadrangular cartilage, perpendicular plate of the ethmoid bone, and the vomer. The authors will then quilt the mucoperichondral flaps with through and through chromic gut or vicryl rapide sutures.
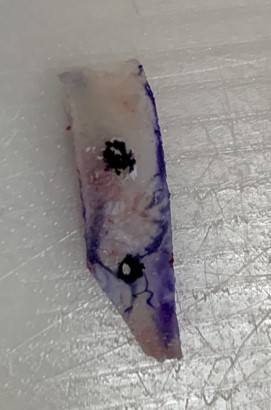
The cartilage and bony parts of the septal graft can be used as a continuous piece or separately. When using the bony septum, an 18 gauge needle can be used to create holes in the bony graft to allow sutures to pass through. (Figure 2) Bony spurs can be corrected with a 4mm burr. In addition, thicker areas of bone can be contoured to create a thin plate that will create a scarf joint with the caudal septum with the most caudal end of the septal extension graft in the midline.
Applications
The harvested osteocartilaginous septal graft can be utilized in many ways depending on what is required. The bony and cartilaginous components can be separated to create different grafts, or kept in unit as a composite graft. The bony septal graft is best used as structural grafts given the rigidity and strength of the bony septum. These grafts are most commonly used as spreader grafts or caudal septal extension grafts. (Figure 3 and 4) More rarely, they can be used as lateral crural strut or alar batten grafts. They do not function well as camouflage grafts, tip or shield grafts, or small grafts. Others have described their use in Asian rhinoplasty as septal extension grafts. [3, 4, 5] The holes in the bony graft should not be placed too close together to prevent fracture of the bone, as such, bony septal grafts have to be large enough to incorporate the suture holes.
Conclusion
In rhinoplasty where complex or significant structural or reconstructive grafting is required, maximizing the amount of grafting material is essential. Autografts are excellent choices for use in rhinoplasty. By utilizing both the cartilaginous and bony septum, additional grafting material can be created. It is important, however, to recognize the quality of the grafting material to use them to their maximum potential.
References
- Kim JS, Khan NA, Song HM, Jang YJ. Intraoperative measurements of harvestable septal cartilage in rhinoplasty. Ann Plast Surg. 2010;65(6):519-23.
- Onerci TM, Ayhan K, Oğretmenoğlu O. Two consecutive cases of cerebrospinal fluid rhinorrhea after septoplasty operation. Am J Otolaryngol. 2004;25(5):354-6
- Kim GR, Park K, Kim T. Use of nasal septal bone for septal extension graft after jaw surgery. Plast Reconstr Surg Glob Open. 2013;1(8):e76.
- Lee SH, Koo MG, Kang ET. Septal Cartilage/Ethmoid Bone Composite Graft: A New and Improved Method for the Correction Underdeveloped Nasal Septum in Patients with Short Noses. Aesthetic Plast Surg. 2017;41(2):388-394.
- Ahn TH, Zheng T, Kang HJ, Yoo BJ, Chung JH, Jeong JH. New Technique in Nasal Tip Plasty: Sandwich Technique Using Cartilage and Septal Bone Complex. Ear Nose Throat J. 2019;:145561319881570.
Figures Legend




Disclosures:
The authors have no conflicts of interests or financial interests with respect to the authorship and/or publication of this article