Nasal septal deviation is one of the primary causes of nasal obstructions.
The septal deviations can interested caudal, dorsal or both caudal and dorsal segments.
The aim of this paper is to suggest a suitable diagnostic work-up of the nasal obstruction and describe some technical surgical procedures that can be used for different nasal septum deviation types and severities
Septum deviation is one of the most common nasal conditions, causing problems such as obstruction, scabbing, nosebleed, and poor sleep quality.
In most cases, the nasal septum is not perfectly aligned with the midline, and deviations or irregularities are present. Although a nasal septum deviation might have post-traumatic or iatrogenic origins, it is known that its etiology is commonly congenital. In fact, in a recent study, Harugo et al. demonstrated that a significant nasal deviation is present in almost 20% of infants (1).
Nasal deviations become clinically significant when their functional impact is such that it affects the quality of life.
After tonsillectomy, septoplasty is the surgical procedure performed most frequently in the head and neck areas and, for this reason, it is frequently also done by young surgeons. However, as with every surgical practice, there are several issues from a technical and surgical point of view.
The submucous resection of bone spurs or deflected cartilage is not complicated in itself. However, at least 1-1.5cm of dorsal and caudal septal cartilage must be saved in order to avoid saddle nose or nasal ptosis. Therefore, if the deviation affects these quadrangular cartilage areas, it is not sufficient to remove them, but it is also necessary to reinforce or reconstruct them after the appropriate correction.
The aim of this paper is to suggest a suitable diagnostic work-up of the nasal obstruction and describe some technical surgical procedures that can be used for different nasal septum deviation types and severities.
Surgical Anatomy
It is important to highlight some anatomical details which are useful from a surgical standpoint. In particular, the term “L-strut”refers to the “L” shape of the septum structure, i.e. the dorsal and caudal cartilaginous septum supporting the nasal pyramid.
The caudal segment of the septum contributes to supporting the nasal tip, determining its projection, and is important for the functioning of the internal and external nasal valves. This segment has a strong relationship with the anterior nasal spine (ANS) and a weak relationship with the membranous septum and medial crura. The relationship between the ANS and the posterior septal angle is crucial in that it provides further support for the nasal tip. A weakening or reduction of the caudal septum or its separation from the ANS could cause a ptosis of the nasal tip. Stenosis of the internal nasal valve is another major consequence caused by caudal septal deviation (2).
The dorsal segment of the septum defines the third medium of the nose, together with the triangular cartilages. Its alteration could lead to “C”- or “S”-shaped deviations of the nose. It also defines the internal nasal valve.
The K-area, or Keystone area, is the convergence point of the triangular cartilages, nasal bones, and osseous and cartilaginous septa. This area is considered one of the most important for the nasal support, and its alteration or iatrogenic or post-traumatic interruption may cause saddle nose or a dorsal line modification (e.g. “reversed V” shape deformity).
It is obvious that the caudal and dorsal segments of the septum play an important role as far as both function and aesthetic appearance are concerned, so they must be preserved or rebuilt if they become weakened or deviated. If the deviation involves the caudal and dorsal septum, cartilaginous grafts are necessary for strengthening purposes(3).
Surgery Of The Caudal Septal Deviations
Different classifications of caudal septal deviations have already been described.
In the classification proposed by Apaydin (4), caudal deviations are classified on the basis of their severity: subluxation, concave, retracted, fractured, and missing caudal segment. For each category, the following surgical solutions are proposed:
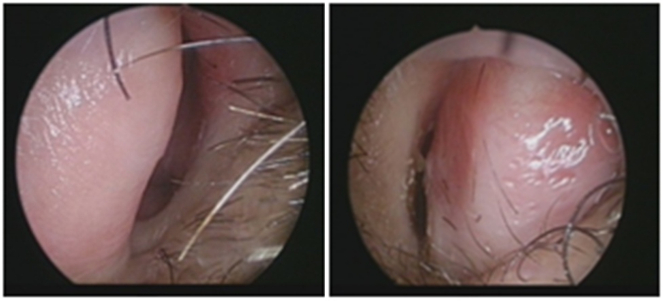
- Subluxation: In this case it is sufficient to reposition the septum by securing it to the nasal spine, after an appropriate dissection and remodeling. If the nasal structure has to be reinforced or the nasal tip has to be corrected by derotation, whether or not combined with a columellar show, the tongue-in-groove technique can be useful (5) (Fig. 1).
- Concave: Some authors suggest either cutting incomplete incisions or making horizontal multiple sutures on the concave side (6) (Fig. 2). These surgical techniques may be inadequate for nasal correction and may sometimes cause a weakening of the anterior nasal support, resulting in nasal tip ptosis. According to Apaydin, it is necessary to splint the concave side of the caudal segment with a batten graft. The graft can be obtained from cartilage or a bone layer which is perpendicular to the ethmoid bone. In the most serious concavities, it is necessary to use a septal extension graft (Fig. 3): this makes it possible to improve the structure of the caudal segment and the nasal tip, while correcting the concavity. This technique secures the graft to the caudal segment edge, which was previously connected to the ANS.


- Retraction: In the case of a retracted caudal segment caused by a trauma or previous surgery, it is important to rebuild the nasal septum with an extended columellar strut, which can be either secured end-to-end or overlapped over the residual septum (Fig. 4).
- Fractured: (Fig. 5) Splinting is rarely the appropriate solution for correcting a caudal segment fracture. The deviated part must be removed and rebuilt with a caudal septal replacement graft (Fig. 6) secured to the dorsal segment and the anterior nasal spine, when the batten graft is not sufficient.



- Missing caudal segment: A missing caudal segment may be caused by a serious trauma or previous surgery. It must be reconstructed using a caudal septal replacement graft, which is secured to an extended spreader graft. Rib or conchal cartilage may be needed if septal cartilage is insufficient.
The types of caudal septal deviations and corresponding solutions are summarized in Table 1.
Surgery Of Dorsal Septal Deviations
The deviation of the dorsal segment can determine a “C” or “S” nose deformity, in addition to impacting the internal nasal valve. In this type of deviation, the surgeon must both correct the septal deviation and reconstruct the nasal third medium with the spreader graft.
This consists of a cartilaginous graft of variable height and width, to be positioned between the triangular and dorsal edges of the quadrangular cartilages in order to improve the amplitude of the internal nasal valve and align the dorsal segment (Fig. 7).
The graft can be unilaterally positioned on the convex side in combination with incisions on the concave side. Alternatively, the spreader graft can be used bilaterally. In this case two asymmetrical grafts must be used, the larger of which must be positioned on the concave side.
In the case of linear deviation, the grafts must be positioned on the opposite site of the deviation.
The spreader graft and triangular cartilages must always be secured in order to improve the stability of the dorsal third medium. The spread graft is easily positioned via an open approach, but this can also be done endonasally, as initially described by Sheen (7).
The spreader crossbar graft technique is recommended for a “C”- or “S”-shaped nose, as described by Boccieri (8).

Complex Septal Deviations
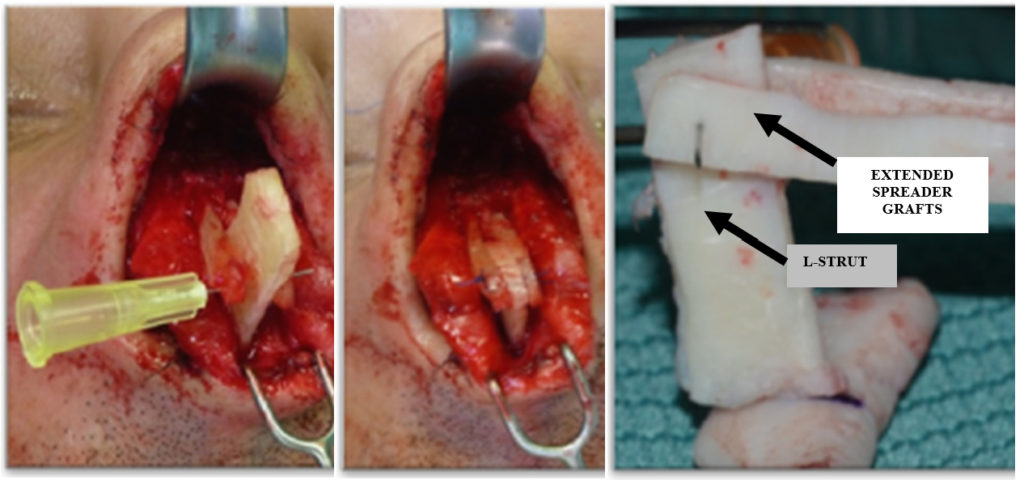
Complex deviations are deviations involving both the caudal and the dorsal septum segment. In these cases, it is necessary to reconstruct both segments with an extended spreader graft and a caudal septal replacement graft (Fig. 8). If possible, a small part of the dorsal strut must be left in the K-area as a reconstruction guide.
Materials And Techniques
This study focuses on surgical operations on patients who underwent functional septoplasty or septorhinoplasty performed by a single surgeon between January 2014 and September 2018. The number of patients considered is 451, with 380 primary cases and 71 revisions.
In almost 80% of the revisions, the nasal obstruction was determined by an excessive reduction of the quadrangular cartilage, with nasal tip ptosis and further failure of the internal valve.
The study considers the following parameters relating to primary case patients:
- % of deviations involving the septal L-strut (caudal deviation, dorsal deviation, and both);
- Evaluation of caudal deviations per Apaydin’s classification and their percentage;
- Analysis of complications.
Results
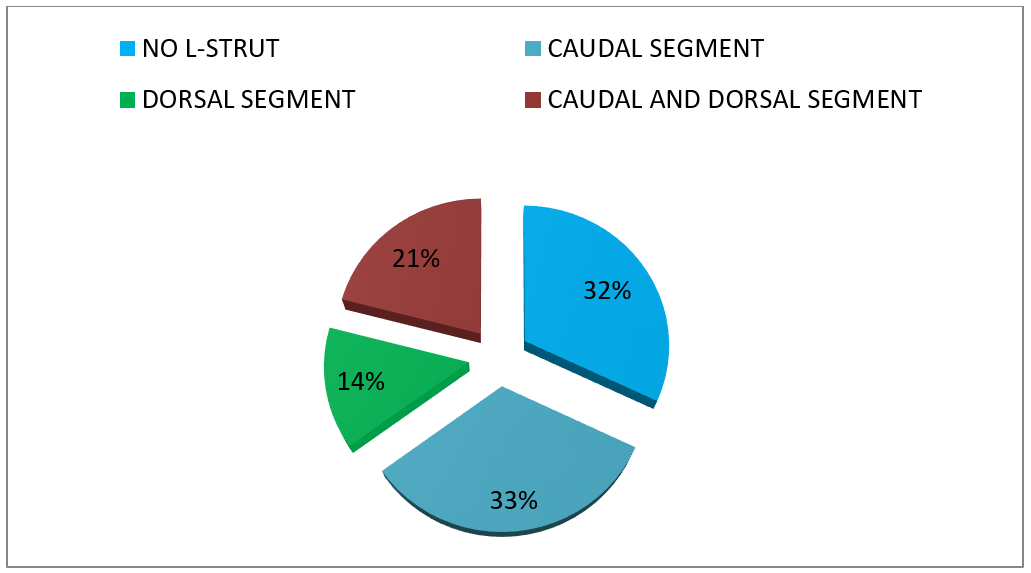
68% (257) of the primary case patients had deviations involving the L-strut.
In particular, considering the total number of primary case patients, the following percentages of deviation types were recorded:
- 33% caudal segment;
- 14% dorsal segment;
- 21% both caudal and dorsal segments. (Fig. 9)
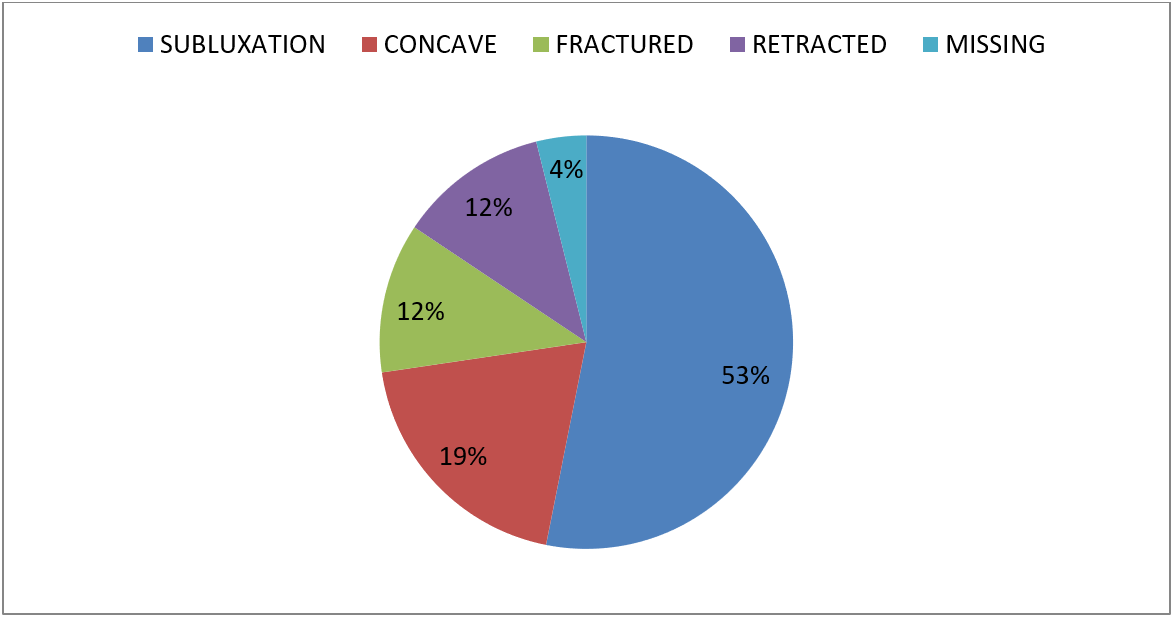
Furthermore, as for the primary cases involving the caudal segment only, the patients may be broken down, per Apaydin’s classification, as follows:
- Subluxation: 68 patients (53%);
- Concave: 25 patients (19%);
- Fractured: 15 patients (12%);
- Retracted: 15 patients (12%);
- Missing : 5 patients (4%). (Fig.10)
As for the post-operative conditions, only 6 complications were detected among all 380 patients (1.5%). There were2 epistaxes, and 1 case of infection with pus drainage, which was successfully treated via combined antibiotic therapy (amoxicillin-clavulanate and levofloxacin) administered for 10 days. The graft was partially dislocated in 3 cases: 2 of them had neither functional nor aesthetical alterations, whereas the third required a surgical revision.
Conclusions
Septoplasty, a common practice in the ENT field, is not always sufficient for solving respiratory problems. The main reasons for its failure may be either inflammatory or anatomical, i.e.in the case of an untreated or persistent nasal deviation.
In particular, in the first case, septoplasty is a type of surgery which cannot be definitive if a patient with a nasal deviation has not been diagnosed with a rhinopathy. For this reason, it is suggested that allergic rhinitis tests be performed on patients prior to any nasal surgery.
In the second case, persistent anatomical obstructions may be due to the following causes:
- Residual septal deviation;
- Internal and/or external valve failure (untreated because it was not diagnosed during the preoperative phase);
- Internal and/or external iatrogenic valve failure;
- Synechia;
- Nasal tip ptosis due toa weakening or resection of the caudal segment.
Septoplasty may consist of either the simple removal of septal spurs with a consequent repositioning of the septum or more complex cartilaginous grafts.
When the L-strut is involved in a septal deviation, cartilage removal procedures are far less effective than reconstruction procedures. It is important to correctly determine the specific type of septal nasal deviation in order to plan the most appropriate surgical procedure.
External palpation should be performed to evaluate the nasal tip and structure during the preoperative phase. If the nasal tip appears compressible, an inadequate septal structure may be assumed.
In the case of caudal deviations, we consider it essential, from the technical standpoint, to secure the posterior septal angle to the anterior nasal spine. With this first reconstruction step, it is possible to stabilize the nasal tip as well as to align the caudal segment.
Afterwards, the septum can be reinforced with cartilaginous grafts, for instance with a batten graft, septal extension graft, and/or extended columellar strut depending on the severity of the defect, based on the above-stated classification. In our opinion, the septal extension graft is the most versatile technique because it is also suitable for endonasal procedures. This kind of graft is very useful when the caudal segment is not only delicate but also shortened, fractured, and/or of a fragile consistency.
The main disadvantage of reconstruction techniques is the longer postoperative healing time. The attachment to the nasal spine and nasal tip rigidity may create a bit of an annoyance for the patient for several months.
As for the dorsal segments of the nasal septum, these can be corrected by spreader grafts. Efficiency is greater if the spreader grafts are positioned after the separation between the quadrangular and the triangular cartilage, as this increases the internal valve angle.
Our experience shows that L-strut deviations are the most frequent (68%);caudal segment deviations are the most numerous among these(33%).
This single-surgeon clinical record reflects the reality of a specialized university center to which patients with complex septal deviations are often referred by other specialists. In our opinion, it is possible that the percentage of L-strut deviations may be lower in common clinical records, but we believe this study provides a good representation of the current situation.
In conclusion, a careful analysis during the preoperative phase, a correct identification of the deformity, and an adequate knowledge of the available surgical techniques must all be considered of fundamental importance, based on our own experience and that of various other authors (9).
| TYPE OF CAUDAL SEPTAL DEVIATIONS | SURGICAL SOLUTIONS |
| SUBLUXATION | Reposition of the septum by securing it to the ANS, after dissection and remodeling |
| CONCAVE | – splint the concave side of the caudal segment with a batten graft -Septal extention graft |
| RETRACTION | Septal extention graft |
| FRACTURED | -Splinting batten graft -Caudal septal replacement graft |
| MISSING CAUDAL SEGMENT | Caudal septal replacement graft (rib or conchal cartilage) |
References
- Harugop AS et Al. Prevalence of Nasal Septal Deviation in New-borns and Its Precipitating Factors: A Cross-Sectional Study.Indian J Otolaryngol Head Neck Surg. 2012 Sep;64(3):248-5.
- Tasca I. La chirurgia funzionale del naso. In: Quaderno monografico di aggiornamento AOOI. Italy. 2007. p 45-69.
- Toriumi DM. Subtotal Septal Reconstruction:An Update. Facial Plast Surg. 2013 Dec;29(6):492-501.
- Apaydin F. Segmental reconstruction for nasal septal deviation. Facial Plast Surg. 2013 Dec;29(6):455-63.
- Kridel R., Scott BA, Foda HM. The tonque in groove technique in septorhinoplasty. Arch Facial Plast Surg. 1999 Oct-Dec;1(4):246-56; discussion 257-8.
- Ellis M. et all. Suture technique for caudal septal deviations. Laryngoscope. 1980 Sep;90(9):1510-2.
- Sheen JH. Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. PlastReconstrSurg. 1984 Feb;73(2):230-9.
- Boccieri A, Pascali M. Septal Crossbar for the correction of the crooked nose. PlastReconstrSurg. 2003 Feb;111(2):629-38.
- Kim DW, Gurney T. Management of nasal-septal L-strut deformities. FacialPlastSurg. 2006 Feb;22(1):9-27.