Abstract
Introduction
The goal of this study report is to define the “gender angle”, a new angle which represent the masculine or feminine nasal shape, for performing a gender-oriented rhinoplasty. The use of the “Gender Angle” in Caucasian patients will help the plastic surgeon in the search for a suitable nose for the patient’s face and above all for the search for maximum patient satisfaction.
Materials and Methods
The study population was obtained from Caucasian patients who had undergone rhinoplasty between January 1986 and September 2016 at our department. Patients answered the Italian version of the FACE-Q outcome instrument on post-rhinoplasty satisfaction with their nose. Anthropometric measurements were performed retrospectively by AutoCAD for MAC on a photograph of the profile view taken postoperatively at the last follow-up.
Results
A total of 1774 (706 male and 1068 female) patients satisfied the inclusion criteria and were finally enrolled in this study. We identified a gender-specific angle ranging from 168° to 182° for the male nose and from 160° to 178° for the female nose. We subdivided all study patients into 3 ranges of angles, as follows: male nose, range 1 = 168°–172°, range 2 = 173°–177°, range 3 = 178°–182°; female nose, range 1 = 160°–166°, range 2 = 167°–171°, range 3 = 172°–178°. All study patients completed the FACE-Q Rhinoplasty postoperative module. Analysis was performed of the FACE-Q results and the angle obtained for each nose. The most satisfactory angle range for the male patients was range 3 (P=0,01) and for the female patients was range 2 (P=0,01).
Conclusions
The “gender angle” might be a parameter that effectively provides the optimal cosmetic result for male and female patients who undergo rhinoplasty.
Level of evidence
Level V: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.
Manuscript
Introduction
Since the nose is located in the center of the face, changes in its external morphology lead to changes in facial features (1–5). The nose should match the patient with regard to the patient’s nationality, gender, ethnicity, and cultural factors that influence the desires of patients (6). Utilizing a 30-year experience with rhinoplasty surgery in our department, we undertook a review of all rhinoplasties performed in our department, and identified an angle that varied based on gender, which had not been previously described in the literature.
Data on the importance of a new measurement of the nasal angle should be introduced, which will aid in the development of plastic surgery, which will improve rhinoplasty care and procedures.
The use of the “Gender Angle” in Caucasian patients will help the plastic surgeon in the search for a suitable nose for the patient’s face and above all for the search for maximum patient satisfaction.
Materials and methods
This retrospective study population was obtained from the Caucasian patients who had undergone rhinoplasty between January 1986 and September 2016 by the same plastic surgeon. Patients answered the Italian version of the FACE-Q rhinoplasty module (7,8). We administered the questionnaire electronically at least 2 years after the surgical procedure for each patient.
All included study patients had undergone primary rhinoplasty for functional or cosmetic problems, had been followed for almost 2 years, had been photographed for a standard postoperative profile image, had a good understanding of the Italian language, accepted to answer to FACE-Q rhinoplasty module, and signed a consent form for inclusion in the study.
Photograph setting
On the basis of the medical literature and our own experience, we follow general criteria concerning patient preparation and positioning as well as camera setting (9-16). We used a single-lens reflex with a fixed focal length of 35 to 70 mm which guarantees an undistorted image. The photographer (plastic surgeron) is obliged to stand at a distance from the subject that allows correct image capture within the preestablished anatomic boundaries, and this is an ideal condition for achieving standardization. We studied the lateral view pictures: From the frontal view, with the patient s whole body rotated 90 ° so as to align the nasal tip and chin. The head must be in its anatomic position with no lateral inclination, neither flexion nor extension. The Frankfurt plane is held horizontal, and the contralateral eyebrow is not visible.
Anthropometric measurements
Anthropometric measurements were performed by one of the author of the study retrospectively by AutoCAD for MAC (Copyright © 2019 Apple Inc. US) (17), on a photograph of the profile view taken postoperatively only at the last follow-up (so only one measurement for each patient). We identified the gender angle as follows: 1) on the lateral view, a line was drawn from the nasion (A) to the supratip break (B); 2) a second line was drawn from the supratip break (B) to the nasal tip (C). The angle between the AB and BC lines was defined as the “gender angle” (Fig. 1). The position of the nasion was set at the level of the supratarsal fold of the upper eyelid. The nasal tip projection was measured on the profile view with the use of Goode’s method. We used AutoCAD software to calculate the angle, and the data were collected and stored in an EXCEL file (© Microsoft 2019). Two plastic surgeons reviewed all postoperative photos of the study patients sample and rated the photos according to a Visual Analog Scale (VAS) of 1 to 5 (1= very bad, 2= poor, 3= adequate, 4= good, 5= very good).
Statistical Analysis
The results obtained from this judgment were correlated with calculated angle ranges. The Fisher exact test was used to compare the groups. P < 0.05 was considered significant.
Results
A total of 1774 (706 male and 1068 female) patients satisfied the inclusion criteria and were finally enrolled in this study. The mean patient age was 34.2 years (range, 18–65 years). The mean follow-up time was 3.7 years (range, 2–12 years). All patients underwent primary rhinoplasty. Demographic data and surgical details are shown in Table 1. We identified a gender angle ranging from 168° to 182° for the male nose and from 160° to 178° for the female nose. We subdivided all study patients into 3 ranges of angles, as follows: male nose, range 1 = 168°–172°, range 2 = 173°–177°, range 3 = 178°–182°; female nose, range 1 = 160°–166°, range 2 = 167°–171°, range 3 = 172°–178°. All study patients completed the FACE-Q Rhinoplasty postoperative module. Analysis was performed of the FACE-Q results and the angle obtained for each nose. The most satisfactory angle range for the male patients was range 3 and for the female patients was range 2 (Table 2, Figure 2). According to evaluations by the 2 reviewers, angle range 3 and angle range 2 were the most satisfactory posoperative results for the male and female patients, respectively (Table 3, Figure 3).
Discussion
The shape of the nose is determined based on a certain number of geometric parameters (angles, curves, and dimensions) and of depressions, nicks, and grooves. Are there any dimensions and proportions that could be considered ideal and which the surgeon could apply during a rhinoplasty? (18). Few papers on anthropometric studies of the nose have been published. As Springer et al (19) affirmed, ideal female noses showed a horizontally and vertically lower nasion and were concave to straight in profile, compared with optimal male noses, which had a vertically and horizontally higher nasion and a straight profile. We agree with these authors and we respect these parameters. There are many important differences between the male and female nose that should be considered (20). The female nose has a smaller bony framework than the male nose, and the dorsum is narrower, with an age-dependent concavity, male noses are usually larger and longer, have broader nasal bones, and the dorsum is straighter, with very little supratip break (21,22). The nasolabial and nasofrontal angles are both more obtuse in the female nose than in the male nose. The nostrils and the nasal base are smaller in the female nose (23–27). Carvalho et al (28) presented a study on anthropometric factors in the Caucasian nose and concluded that facial asymmetries are very common in patients seeking rhinoplasty, and special attention should be paid to such aspects both for surgical planning and for patient counseling. Choi et al (29) used a three-dimensional simulation program for rhinoplasty that allowed an intuitive, rapid, and accurate fabrication of implants, irrespective of the level of surgeon experience. Sarraf-Berger et al (30) presented their experience in the following paper: Comparison of the Preoperative and Postoperative Anthropometric Nose Measurements in the Prospective Study of the Surgical Techniques Used in Primary Rhinoplasty on the Caucasian Nose. The studied angles reported in the literature include the following: nasofacial, nasofrontal, septal, columellar-apical, and nasolabial angle. With our experience, we also noticed that the course of the back between males and females changed to form an angle. Based on our observation, we decided to measure the angles obtained in 1774 patients undergoing rhinoplasty to investigate gender-based differences between the angles. The limitations of our study were: monocentric and retrospective study, cross-sectional and no baseline (pre-surgery) quality of life measures were used, study population were not randomized, no control group was used.
Conclusions
We identified the 2 ranges of nasal angles that were associated with masculine and feminine appearance. The gender angle might be a parameter that effectively provides the optimal cosmetic result for male and female patients who undergo rhinoplasty. However, it should not be forgotten that the shape of the nose must also correspond to other facial features of the patient.
COMPLIANCE WITH ETHICAL STANDARDS
This study was approved by the Ethics Committee of our University. This article contain studies on human participants performed by any of the authors and each subject provided informed written consent before participating in the study. The authors have not Conflict of Interest.
References:
- Barone M., Cogliandro A., Persichetti P. Preoperative symptoms of body dysmorphic disorder determine postoperative satisfaction and quality of life in aesthetic rhinoplasty. Plast Reconstr Surg. 2013 Dec;132(6):1078e-9e
- Barone M, Cogliandro A, Cagli B, Persichetti P. FACE-Q Scales for Health-Related Quality of Life, Early Life Impact, Satisfaction with Outcomes, and Decision to Have Treatment: Development and Validation. Plast Reconstr Surg. 2015;136:272-273.
- Cogliandro A, Barone M, Persichetti P. Italian Linguistic Validation of the FACE-Q Instrument. JAMA Facial Plast Surg. 2017 Jul 1;19(4):336-337.
- Barone M, Cogliandro A, Di Stefano N, Tambone V, Persichetti P. A Systematic Review of Patient-Reported Outcome Measures Following Transsexual Surgery. Aesthetic Plast Surg. 2017 Jun;41(3):700-713.
- Barone M, Cogliandro A, Persichetti P. Role of Rhinoplasty in Transsexual Patients. Plast Reconstr Surg. 2017 Jun;41(3):700-713.
- Barone M., Cogliandro A., Persichetti P. Rhinoplasty: a cross cultural analysis Plast Reconstr Surg. 2013; 132(4):664e-665e
- Barone M, Cogliandro A, Di Stefano N, Aronica R, Tambone V, Persichetti P. Linguistic validation of the “FACE-Q Rhinoplasty Module” in Italian. Eur Arch Otorhinolaryngol. 2017;274(3):1771-1772.
- Klassen AF, Cano SJ , East CA , Baker SB , Badia L , Schwitzer JA , Pusic AL. Development and Psychometric Evaluation of the FACE-Q Scales for Patients Undergoing Rhinoplasty. JAMA Facial Plast Surg. 2016; 18(1): 27-35
- DiBernardo BE, Adams RL, Krause J, Fiorillo MA, Gheradini G: Photographic standards in plastic surgery. Plast Reconstr Surg 102:559_568, 1998
- DiSaia JP, Ptak JJ, Achauer BM: Digital photography for the plastic surgeon. Plast Reconstr Surg 102:569_573, 1998
- Galdino GM, Swier P, Manson PN, Vander Kolk CA: Converting to digital photography: A model for a large group or academic practice. Plast Reconstr Surg 106: 119_124, 2000
- Galdino GM, Vogel JE, Vander Kolk CA: Standardizing digital photography: It_s not all in the eye of the beholder. Plast Reconstr Surg 108:1334_1344, 2001
- Krause JL: Digital photographic standards. Plast Reconstr Surg 112:1177_1178, 2003
- Price MA, Goldstein GD: The use of a digital imaging system in a dermatology surgery practice. Dermatol Surg 23:31_32, 1997
- Rhodes ND, Southern SJ: Digital operation notes: A useful addition to the written record. Ann Plast Surg 48:571_573, 2002
- Yavuzer R, Smirnes S, Jackson IT: Guidelines for standard photography in plastic surgery. Ann Plast Surg 46:293_300, 2001
- https://www.autodesk.com/products/autocad/overview
- Barone M, Cogliandro A, Persichetti P. Patient-reported outcome measures following rhinoplasty. Plast Reconstr Surg. 2018 Jul 19. doi: 10.1097/PRS.0000000000004743. [Epub ahead of print]
- Springer IN, Zernial O, Nölke F, Warnke PH, Wiltfang J, Russo PA, Terheyden H, Wolfart S. Gender and nasal shape: measures for rhinoplasty. Plast Reconstr Surg. 2008;121:629-37.
- Morrison SD, Vyas KS, Motakef S, Gast KM, Chung MT, Rashidi V, Satterwhite T, Kuzon W, Cederna PS. Facial Feminization: Systematic Review of the Literature. Plast Reconstr Surg. 2016; 137: 1759-70.
- Habal MB. Aesthetics of feminizing the male face by craniofacial contouring of the facial bones. Aesthetic Plast Surg. 1990;14:143–150.
- Hage JJ, Becking AG, de Graaf FH, Tuinzing DB. Gender- confirming facial surgery: Considerations on the masculinity and femininity of faces. Plast Reconstr Surg. 1997;99:1799–1807.
- Dempf R, Eckert AW. Contouring the forehead and rhinoplasty in the feminization of the face in male-to-female trans- sexuals. J Craniomaxillofac Surg. 2010;38:416–422.
- Noureai SA, Randhawa P, Andrews PJ, Saleh HA. The role of nasal feminization rhinoplasty in male-to-female gender reassignment. Arch Facial Plast Surg. 2007;9:318–320.
- Altman K. Facial feminization surgery: Current state of the art. Int J Oral Maxillofac Surg. 2012;41:885–894.
- Bartlett SP, Wornom I III, Whitaker LA. Evaluation of facial skeletal aesthetics and surgical planning. Clin Plast Surg. 1991;18:1–9.
- Barone M, Cogliandro A, Di Stefano N, Tambone V, Persichetti P. A Systematic Review of Patient-Reported Outcome Measures Following Transsexual Surgery. Aesthetic Plast Surg. 2017 Jun;41(3):700-713.
- Carvalho B, Ballin AC, Becker RV, Berger CA, Hurtado JG, Mocellin M. Rhinoplasty and facial asymmetry: Analysis of subjective and anthropometric factors in the Caucasian nose. Carvalho B, Ballin AC, Becker RV, Berger CA, Hurtado JG, Mocellin M. Int Arch Otorhinolaryngol. 2012;16:445-51.
- Choi YD, Kim Y, Park E. Patient-Specific Augmentation Rhinoplasty Using a Three-Dimensional Simulation Program and Three-Dimensional Printing. Aesthet Surg J. 2017 Oct 1;37(9):988-998.
- Berger CA, Freitas Rda S, Malafaia O, Pinto JS, Macedo Filho ED, Mocellin M, Fagundes MS. Prospective study of the surgical techniques used in primary rhinoplasty on the caucasian nose and comparison of the preoperative and postoperative anthropometric nose measurements. Int Arch Otorhinolaryngol. 2015;19:34-41.
Table:
Table 1: population data
| Number (N=1774) | |
| Age | |
| Mean (years old) | 34,2 |
| Gender | |
| Male | 706 |
| Female | 1068 |
| Follow up | |
| Mean (years) | 3,7 |
| Septal Deviation type | |
| C-Shape | 910 |
| S-shape | 802 |
| None | 62 |
| Type of access | |
| Open | 1062 |
| Closed | 712 |
| Type of Dorsum Grafts (male) | |
| Dorsal onlay graft | 65 |
| Dorsal sidewall onlay graft | 32 |
| Radix graft | 10 |
| Spreader grafts | 324 |
| Septal extension grafts | 234 |
| none | 41 |
| Type of Dorsum Grafts (female) | |
| Dorsal onlay graft | 76 |
| Dorsal sidewall onlay graft | 28 |
| Radix graft | 18 |
| Spreader grafts | 542 |
| Septal extension grafts | 246 |
| none | 158 |
| Type of Tip Grafts (male) | |
| Columellars Strut | 256 |
| Onlay tip graft | 152 |
| Shield graft | 81 |
| Subdomal graft | 21 |
| Umbrella graft | 107 |
| none | 109 |
| Type of Tip Grafts (female) | |
| Columellars Strut | 302 |
| Onlay tip graft | 416 |
| Shield graft | 123 |
| Subdomal graft | 65 |
| Umbrella graft | 156 |
| none | 69 |
| Average time between the last operation and completing the questionnaires (months) | 48 |
Table 2: FACE-Q Satisfaction with the nose post operative module for male and female patients
| FACE-Q Satisfaction with the nose post operative module for male patients | Range 1
(N=116) | Range 2
(N=289) | Range 3
(N=301) | P 1-2 | P2-3 | P 1-3 |
| The width of your nose at the bottom (from nostril to nostril)? | 86 (74%) | 211 (73%) | 287 (95%) | 0,87 | <0,01† | <0,01† |
| The length of your nose? | 69 (59%) | 212 (73%) | 297 (99%) | 0,03† | <0,01† | <0,01† |
| How the bridge of your nose looks (where glasses sit)? | 69 (59%) | 232 (80%) | 299 (99%) | <0,01† | <0,01† | <0,01† |
| How well your nose suits your face? | 65 (56%) | 225 (78%) | 298 (99%) | <0,01† | <0,01† | <0,01† |
| How straight your nose looks? | 66 (57%) | 221 (76%) | 297 (99%) | <0,01† | <0,01† | <0,01† |
| The overall size of your nose? | 65 (56%) | 210 (73%) | 285 (95%) | 0,01† | <0,01† | <0,01† |
| The shape of your nose in profile (side view)? | 54 (46%) | 209 (72%) | 299 (99%) | <0,01† | <0,01† | <0,01† |
| How your nose looks in photos? | 55 (47%) | 211 (73%) | 299 (99%) | <0,01† | <0,01† | <0,01† |
| How the tip of your nose looks? | 54 (46%) | 209 (72%) | 285 (95%) | <0,01† | <0,01† | <0,01† |
| How your nose looks from every angle? | 60 (52%) | 208 (72%) | 284 (94%) | <0,01† | <0,01† | <0,01† |
| FACE-Q Satisfaction with the nose post
operative module for female patients | Range 1
(N=247) | Range 2
(N=395) | Range 3
(N=426) | P 1-2 | P2-3 | P 1-3 |
| The width of your nose at the bottom (from nostril to nostril)? | 220 (89%) | 390 (99%) | 337 (79%) | <0,01† | <0,01† | 0,05 |
| The length of your nose? | 219 (88%) | 389 (98%) | 331 (78%) | <0,01† | <0,01† | 0,05 |
| How the bridge of your nose looks (where glasses sit)? | 219 (88%) | 389 (98%) | 330 (77%) | <0,01† | <0,01† | 0,04† |
| How well your nose suits your face? | 221 (89%) | 391 (99%) | 324 (76%) | <0,01† | <0,01† | 0,01† |
| How straight your nose looks? | 222 (90%) | 388 (98%) | 329 (77%) | 0,02† | <0,01† | 0,01† |
| The overall size of your nose? | 221 (89%) | 389 (98%) | 322 (76%) | <0,01† | <0,01† | 0,01† |
| The shape of your nose in profile (side view)? | 223 (90%) | 391 (99%) | 333 (78%) | <0,01† | <0,01† | 0,02† |
| How your nose looks in photos? | 222 (90%) | 391(99%) | 339 (80%) | <0,01† | <0,01† | 0,04† |
| How the tip of your nose looks? | 221 (89%) | 391 (99%) | 341 (80%) | <0,01† | <0,01† | 0,07 |
| How your nose looks from every angle? | 223 (90%) | 388 (98%) | 339 (80%) | <0,01† | <0,01† | 0,04† |
*Raw score ≥ 3.
†Statistically significant.
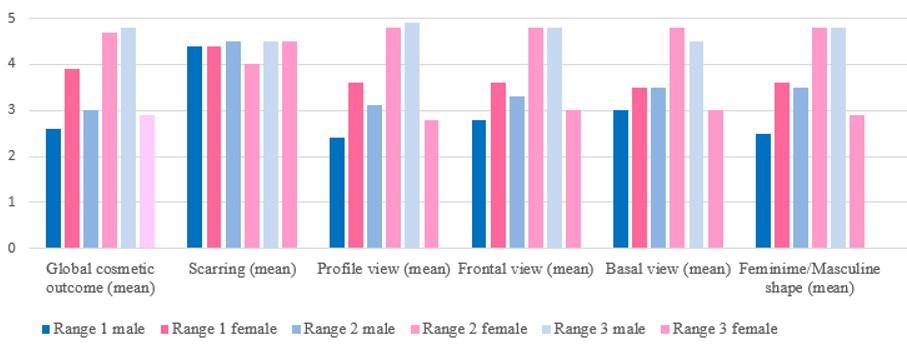
Table 3: Surgeons reviewers VAS Scale for male and female patients
| VAS Scale for male patients | Range 1
(N=116) | Range 2
(N=289) | Range 3
(N=301) | P 1-2 | P2-3 | P 1-3 |
| 2,6 | 3,0 | 4,8 | 0,4 | <0,01† | <0,01† |
| 4,4 | 4,5 | 4,5 | 0,7 | 1 | 0,7 |
| 2,4 | 3,1 | 4,9 | 0,1 | <0,01† | <0,01† |
| 2,8 | 3,3 | 4,8 | 0,3 | <0,01† | <0,01† |
| 3.0 | 3,5 | 4,5 | 0,3 | 0,01† | <0,01† |
| 2,5 | 3,5 | 4,8 | 0,04† | <0,01† | <0,01† |
| VAS Scale for female patients | Range 1
(N=247) | Range 2
(N=395) | Range 3
(N=426) | P 1-2 | P2-3 | P 1-3 |
| 3,9 | 4,7 | 2,9 | 0,02† | <0,01† | 0,03† |
| 4,4 | 4,0 | 4,5 | 0,2 | 0,2 | 0,7 |
| 3,6 | 4,8 | 2,8 | <0,01† | <0,01† | 0,09 |
| 3,6 | 4,8 | 3,0 | <0,01† | <0,01† | 0,2 |
| 3.5 | 4,8 | 3,0 | <0,01† | <0,01† | 0,2 |
| 3,6 | 4,8 | 2,9 | <0,01† | <0,01† | 0,1 |
†Statistically significant.
From 0 to 5 points
Figure:
Figure 1: Anthropometric measurement methods: 1) on the lateral view, a line was drawn from the nasion (A) to the supratip break (B); 2) a second line was drawn from the supratip break (B) to the nasal tip (C). The angle between the AB and BC lines was defined as the “gender angle”
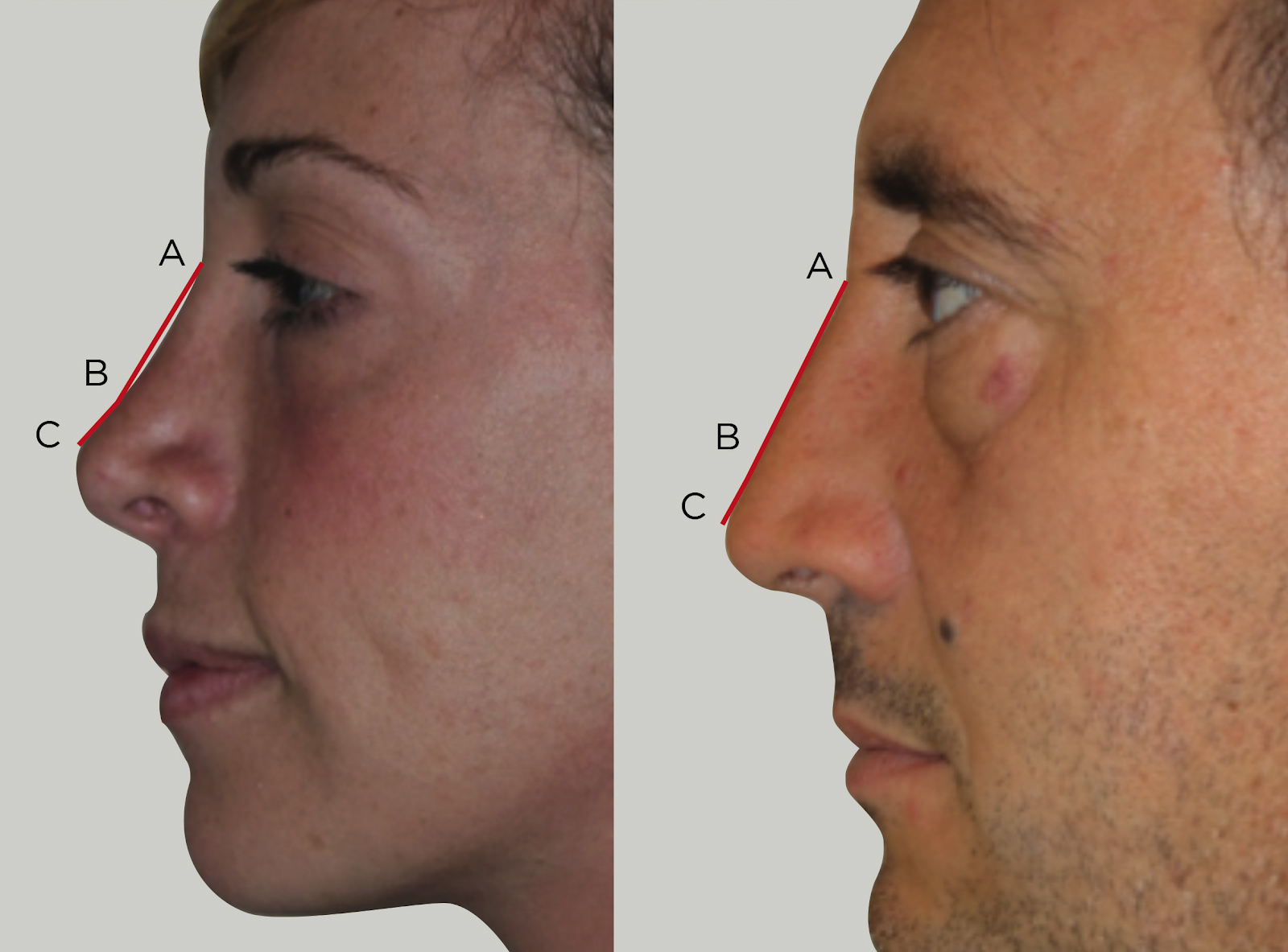
Figure 2: FACE-Q Satisfaction with the nose post operative module for male and female patients
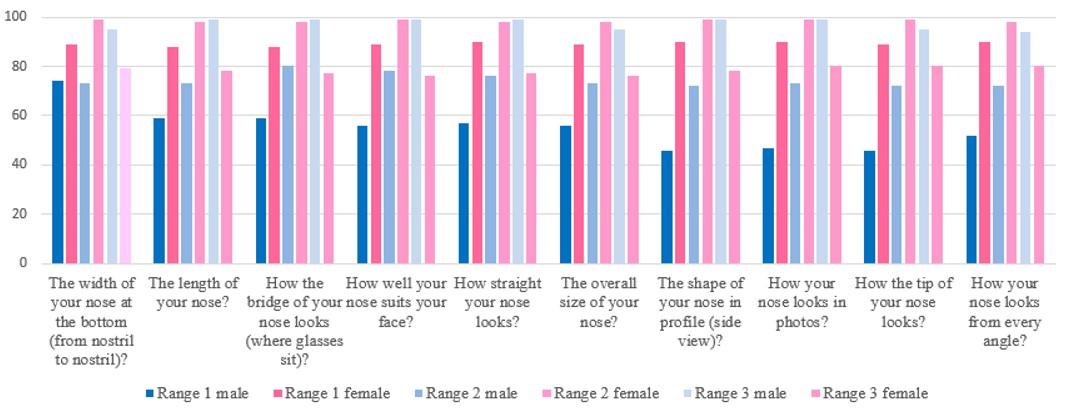
Figure 3: Surgeons reviewers VAS Scale for male and female patients