Chief Complaint
Nasal obstruction and nasal deformity
History of Present Illness
30 year old female presented to the office with complaints of long-standing right > left nasal obstruction. There were no alleviating or aggravating factors. She denied nasal trauma or a history of nasal surgery. Additionally, she had aesthetic concerns regarding her nose. She wanted reduction of the dorsum and elevation of her tip.
Analysis of Photographs

Frontal View:
Proportional horizontal thirds and vertical fifths
Mild dorsal deviation to the right in the middle third
Relatively wide lower third
Irregular brow-tip aesthetic line due to midvault deviation
Symmetric, slightly widened tip defining points
Right alar base more cephalically oriented


Lateral Views:
Radix position adequate
Slight chin underprojection
Excessive dorsal height with dorsal hump
Tip underrotated
(Palpation revealed poor tip support)

With Inspiration

Base View:
Lateral nasal sidewall insufficiency with right external valve collapse
Shortened medial crura
Slightly widened domes
Wide alar base
Intranasal Exam:
Broad based septal deviation to the right
Lateral wall insufficiency with collapse of bilateral internal valves (right > left)
Bilateral inferior turbinate hypertrophy
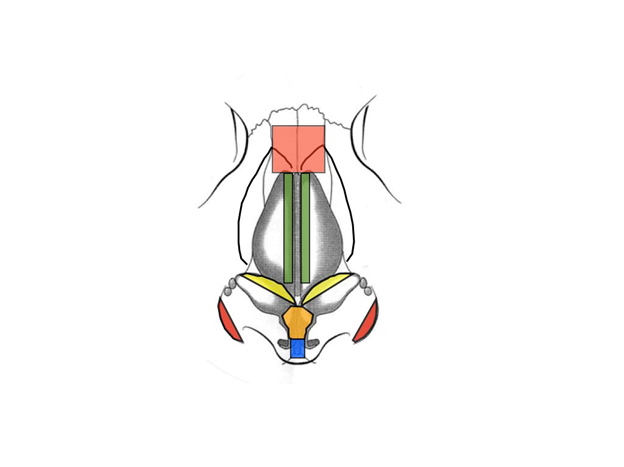
Operative Plan:
Elevate septal flaps
Submucous resection of the inferior turbinates
Open rhinoplasty approach
Septal upper lateral cartilages from the septum
Rasp dorsum
Dorsal cartilaginous reduction
Medial and lateral osteotomies to close open roof
Upper lateral turn in flaps used as bilateral autospreader grafts
Septoplasty
Cephalic trim
Caudal extension graft
Tongue in groove setback of medial crura
Tip graft
Alar base excisions
Intraoperative Photo
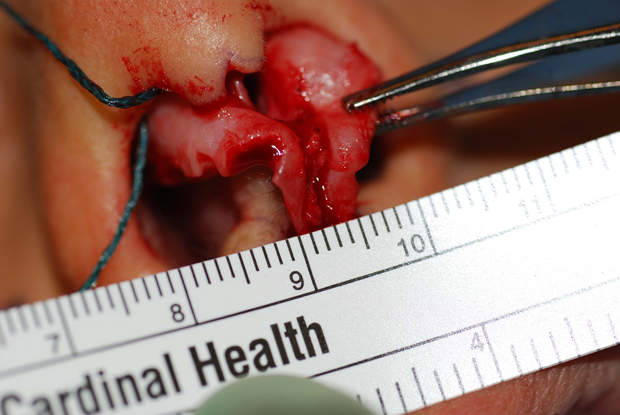
Note the severely atrophic medial crura
9 Month Post-Operative Photos



