Surgery of the Nasal Tip
EXERCISES (Appendix F) Placement of Columellar Strut
The placement of a rectangular cartilage strut between the medial crura can improve tip support and augment tip projection. A columellar strut also can be used to correct buckled medial or intermediate crura or to increase columellar show. The strut may be placed by using the external approach or into a precise pocket via the endonasal approach.
Placement of Columellar Stmt via an External Rhinoplasty Approach
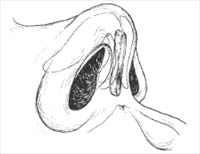
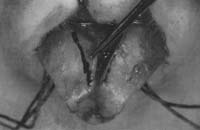
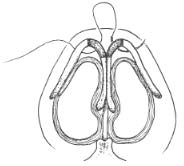
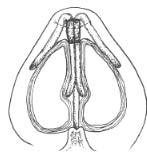
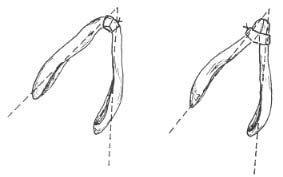
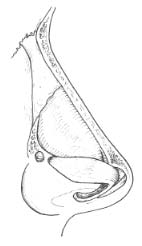
The area between the medial crura is dissected to create a pocket to place the strut. The rect angular cartilage strut typically measures 8 mm to 12 nun in length, 3 mm to 4 min in width, and 1 4 n 4 n to 2 4 nm in thickness. The strut is most typically fashioned from harvested septal cartilage, but also, when necessary, from auricular cartilage, and at times from rib cartilage. The strut is positioned so that it sits above (without extending to) the nasal spine (Fig. 1). It is preferable to leave a small soft-tissue pad between the strut and the nasal spine. The strut should not extend above the intermediate crura. It is secured to the medial crura with several absorbable mattress sutures (e.g., 4-0 plain gut, Keith needle) placed through the vestibular skin. Asymmetries of the lower lateral cartilage (LLC) may be improved with placement of the strut (Fig. 2). Asymmetry of the tip may be created if the medial crura are asymmetrically sutured to the strut (Fig. 3), or if an overlong shut extending beyond the nasal spine shifts to the side of the nasal spine, thereby causing a deviated nasal tip (Fig. 3) (1,2).
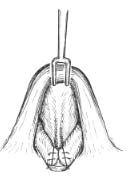
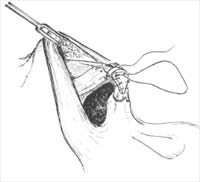
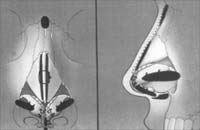
A small incision is made through the vestibular skin and ipsilateral medial crux (Fig. 4). Scissor dissection creates a precise pocket through this small incision (Fig. 5). The columellar strut is inserted into the precise pocket (Fig. 6) and is manipulated into proper po sition (Fig. 7). A 5-0 chromic mattress suture can be used to fix the strut between the me -dial crura. The incision is closed with a single absorbable suture (3).
Figure 1. Placement of columellar strut. A, B: The strut sits above (without extending to) the nasal spine, and it should not extend above the intermediate crura. A columellar strut may be placed via the external rhinoplasty approach. With proper exposure achieved, dissection of a pocket between the medial crura is undertaken. The carved columellar strut is placed in the pocket, as described earlier and secured with interrupted 4-0 plain gut on a straight septal (Keith) needle.


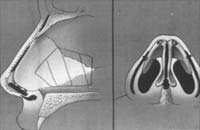
Figure 2. A—D: Asymmetries of the lower lateral cartilage may be improved with placement of the strut.



Figure 3. Asymmetry may be created if the medial crura are.
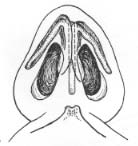
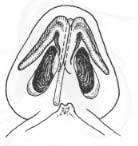
Figure 4. Placement of columellar strut via an endonasal asymmetrically attached to the strut (A), or if an overlong strut approach. First, an incision is made through the vestibular skin extending beyond the nasal spine “slips” to the side of the and ipsilateral medial crus. nasal spine, thereby causing a deviated nasal tip (B).

Figure 5. Scissor dissection creates a precise pocket.
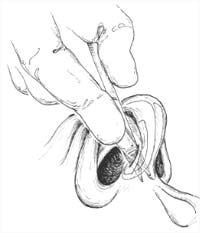
Figure 6. The columellar strut is inserted into the precise pocket.

Identify the Dome
Identify the dome and approximate the lateral and medial crura at the dome with a pair of multitoothed Brown-Adson forceps. The line of the dome should be at approximately 30 degrees to the sagittal plane.
Figure 7. Completed placement of columellar strut via an endonasal approach.
Identify the scroll region. the cephalic border of the LLC (Fig. 8). Excise the cephalic portion of the LLC by making an incision parallel to the caudal margin with the 15 blade and then peeling off the cephalic portion, leaving the vestibular skin behind. The line of incision parallels the caudal margin of the LLC. Leave at least 7 mm to 9 mm of intact cartilage. This preserves an intact strip of cartilage from the feet of the medial crura to the most lateral part of the lateral crux. This will produce conservative narrowing of the nasal tip.
Figure 8. Cephalic resection of lateral crura of lower lateral cartilages.
Now apply domal/transdomal sutures as outlined. Place Individual Horizontal Mattress Domal Sutures
For domal sutures (Fig. 9), a mattress sut u r e of 5-0 polydioxanone suture (I’DS) or other appropriate suture is passed through each dome, and the knot of each mattress suture is tied between the domes. As the sutures are secured, narrowing of the tip is accomplished. An interdomal suture sets the width between the domes. If stiff nasal-tip cartilages are en-countered, the surgeon should use 5-0 clear nylon instead of PDS (4-6).



Place Single Transdomal Suture
Alternatively, a single transdomal suture that t r averses both domes may be placed, in lieu of two individual domal sutures and an interdomal suture (Fig. 10) (1-3). The caudal pass should be slightly longer than the cephalic pass of the mattress suture. When the mattress suture is placed in this fashion, the caudal edge will tend to lead the cephalic edge as the suture is tightened. This creates a more favorable tip-supratip relation. If the cephalic edge leads the caudal edge of the lateral crux despite proper placement of the domal suture, a small cephalic wedge of the cartilage may be excised and the edges sut u r ed, which reposi tions the cephalic edge lower in relation to the caudal edge (Fig. I I ).
Figure 9. Individual horizontal mattress domal sutures. The caudal pass is slightly longer than the cephalic pass of the mattress suture. As the sutures are secured, narrowing of the tip is accomplished. An interdomal suture is placed between the two domes, securing the interdomal distance.
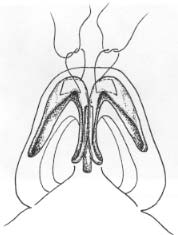
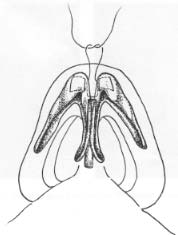
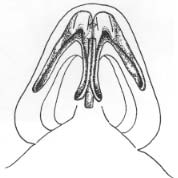
Figure 10. A single transdomal suture may be placed in lieu of two individual domal sutures and an interdomal suture. Patient with trapezoidal tip and broad domal angles. Transdomal suture tech niques were used to improve the patient’s tip triangularity as seen in preoperative and post operative photographs. Patient with trapezoidal asymmetric nasal tip. Columellar strut and transdomal suture techniques were useful to improve tip symmetry and triangularity. Preoperative frontal and base view. Graphic operative worksheet (Gunter diagram). Intraopera tive photographs illustrating placement of columellar strut and suture techniques. Preoperative and postoperative photographs.
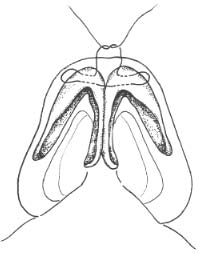
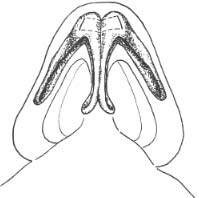


Figure 11. If the cephalic edge leads the caudal edge of the lateral crus despite proper placement of domal suture, a small cephalic wedge of the cartilage may be excised, and the edges sutured, which repositions the cephalic edge lower in relation to the caudal edge. In this figure, one lower lateral cartilage illustrates the wedge excised, and the other illustrates the edges resutured (A). B: The effect of this maneuver on the relationship between the cephalic and caudal edge is illustrated.
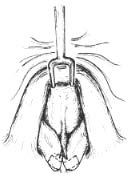

Figure 12. A, B: Lateral crural steal. When the horizontal mattress domal sutures take a larger bite of lateral crus, a portion of the lateral crus is “borrowed” by the medial crus. The “medial crural” leg of the tripod is lengthened, whereas the “lateral crural” legs of the tripod are shortened (see Appendices A and F). This results in increased projection and rotation. Tip refinement also is achieved, as with a standard domal suture. Rotation of this patient’s nasal tip was achieved by using the lateral crural steal tech nique and by suturing medial crura back on overly-long midline caudal septum.
Lateral crural steal (Fig. 12) is an effective method for increasing tip projection and rotation (7). When the horizontal mattress domal sutures take a larger bite of lateral crux, a por tion of the lateral crux is shifted medially. The “medial crural” leg of the tripod is lengthened, whereas the “lateral crural” legs of the tripod are shortened (see Appendices A and F); the result is increased projection and rotation. Tip refinement also is achieved, as with a standard dornal suture.
Further Refinement with Dome Division with Intact Vestibular Skin and Suture Reconstitution
We rarely divide the domes, but when this technique is performed, it is usually in the thick- skinned patient. In most cases, we use some form of dome-binding suture to change tip con -tour (8).
Remove the transdomal sutures to perform this maneuver. Dividing the dome by vertical incision allows further narrowing of the nasal lobule. Projection also can be altered by removal of a superiorly based triangle of cartilage lateral or medial to the vertical incision. By excising a larger amount of cartilage along the cephalic margin of the lateral crux, the cephalic dome can be positioned below the caudal dome (Fig. 13).
Figure 13. Divide the dome by vertical incision. Reapproximate the divided cartilages with suture (e.g., 6-0 PDS) to secure the position of the cartilage and reconstitute the intact strip.
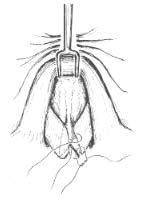

Figure 14. Suture reapproximation of divided lower lateral cartilages is undertaken with simple interrupted stitches. Mattress stitches in this situation may result in overnarrowing.
Reapproximate the divided cartilages with 6-0 PDS suture (Fig. 14). The placement of sutures to reapproximate the divided cartilages after dome division secures the position of the cartilage and contributes to increased tip stability. Simple interrupted sutures are preferred to a mattress suture, because a mattress suture may excessively narrow the tip (Fig. 14).
Note: We rarely perform dome division because we find less-aggressive techniques (dome-binding suture) very effective for modifying tip contour. We try to avoid dome di-vision in patients with thin skin.
Lateral Crural Overlay
When the patient’s anatomy calls for rotation and deprojection, lateral crural overlay is one possible technique (Fig. 15) (7,9). The lateral crura are incised lateral to the domes. The vestibular mucosa is elevated from the undersurface of the lateral crus, and the medial por tion is overlapped over the lateral and secured in place with sutures. When undertaking this maneuver, great care must be taken to perform it symmetrically.
Figure 15. (left and above) A—J: Lateral crural overlay. Great care must be taken to perform this technique symmetrically.










Sutured in place, shield-shaped tip grafts typically are used to increase tip projection and change tip contour (1,2). They also can be used to camouflage tip asymmetries. Tip grafts should be avoided in patients with thin skin.
Carve a shield-shaped tip graft from the harvested septal cartilage. The width generally varies from 8 mm to 12 nun at the leading edge. The length varies from 8 nun to 15 mm, and thickness typically varies from I mm to 3 nun (Fig. 16). The graft is thicker at the leading edge and thinner at the base. One may consider cutting the graft larger at the leading edge to allow in situ carving once the graft is secured in position. The graft is sutured to the caudal margins of the medial/intermediate crura that have been stabilized by the suturedin-place columellar strut. An excessively thick tip graft will increase fullness in the infratip lobule.
Secure the tip graft with 6-0 PISS or Monacryl sutures (Fig. 17). Four to six sutures are usually applied. Place the lower sutures first.
Figure 16. A—E: Tip graft width generally varies from 8 mm to 12 mm at the leading edge. The length varies from 8 mm to 15 mm, and thickness typically varies from 1 mm to 3 mm.




Figure 17. A: The tip graft is sutured to the caudal margins of the medial/intermediate crura. Four to six 6-0 PDS sutures are typically placed. Place the middle sutures first. Intraoperative photographs illustrating placement of tip graft. Preoperative and postoperative photographs of a patient who underwent application of a tip graft. The tip graft was used to increase tip projection and provide a bidomal shape to the nasal tip. Please refer to text for a more detailed discussion of tip grafts.

When placing a tip graft in a patient whose domes have been divided (and suture reconstituted), apply the tip graft so that it camouflages the caudal aspect of the cut domes (Fig. 18), decreasing the risk that this point will be palpable or visible after surgery.
Figure 18. If a tip graft is applied in a patient with divided domes, the caudal aspect of the cut domes should be hidden behind the tip graft to decrease the risk of a palpable or visible point after surgery.
Typically, a tip graft should be projected 1mm to 2mm above the existing domes. In patients with thick skin and an underprojected tip, a longer tip graft can be projected 2 mm to 4 mm above the existing domes. In these and other appropriate cases, a cap or buttress graft placed behind the leading edge of the tip graft may be useful to support the graft (particularly softer, pliable auricular cartilage tip grafts) and to prevent excessive cephalic rotation of the graft under the tension of closure of the skin/soft-tissue envelope. Buttress g rafts are sutured to the tip graft and both domes by using 6-0 PDS or Monaciyl suture (Fig. 19). The buttress grafts should create a smooth transition from the edge of the tip graft to the caudal margin of the lateral crura (2).
Figure 19. Preoperative and postoperative photographs of two patients who had tip grafts with capgraft placement. Cap grafts were placed to support the leading edge of the grafts, prevent cephalic rotation of the graft, and ensure a smooth transition from the edge of the graft to lateral crus. Intraoperative photograph illustrating tip graft with cap graft.


Alar Batten Graft
The external nasal valve is composed of the cutaneous and skeletal support of the mobile alar side-wall. Overaggressive resection of the lateral crura during rhinoplasty and the subsequent postoperative soft-tissue contraction may lead to internal and/or external nasal valve compromise. Cephalic positioning of the lateral crura also will leave suboptimal structural support in the mobile alar side-wall (external valve collapse).
Alar batten grafts, typically of curved septal or auricular cartilage, placed to support the alar rim, can correct internal or external nasal-valve collapse (Fig. 20) (10-12).
Create a precise pocket for an alar batten graft. The graft is typically placed caudal to the lateral crura at the point of maximal lateral nasal wall collapse. Fashion a graft from harvested auricular or septal cartilage, and insert it into the precise pocket. The pocket is sub-cutaneous and is placed at the point of maximal supraalar collapse. Auricular cartilage is preferred because of the cu r vature of the cartilage. The convex side of the graft is oriented laterally to correct the supraalar pinching. If this pocket is too superficial, the graft may be palpable or visible. When placed via an external rhinoplasty approach, secure the graft with a suture applied medially from the graft to adjacent soft tissue or lateral crus.
Figure 20. Alar batten graft. Intraoperative photographs illustrate location of alar batten graft placement, centered around the point of greatest weakness and concavity of the alar sidewall. The alar batten graft in this case has been fashioned with autogenous auricular cartilage. Alar batten grafts may be placed via a precise pocket endonasal rhinoplasty approach. The rhinoplasty worksheet illustrates that this patient underwent septoplasty with cartilage harvest. She underwent conservative cephalic resection. She received a columellar strut, plumping grafts, dorsal onlay grafts, spreader grafts, and alar batten grafts. Preoperative and postoperative photographs are seen here. Note the improvement in the nasal valve, best seen on base view.

Lateral Crural Grafts
Lateral crural grafts are anatomic grafts that replace excessively reduced or deformed lateral crura. These grafts are shaped like lateral crura and measure approximately 5 nun in vertical height. Auricular cartilage has the ideal curvature for lateral crural grafts. The grafts are sutured to the vestibular skin and medial or intermediate crura. Care is taken so the caudal margins of the grafts are placed symmetrically, otherwise. there may be asymmetry of the alar rims. Grafts that are too large or curved may create a bulbous tip (2).
PEARLS
Complete Strip
Although many surgeons perform cephalic trim of the lateral crura as a routine maneuver during rhinoplasty, some patients have flat or concave lateral crura that do not contribute to tip bulbosity. Many of these patients do not need to undergo cephalic trim of the lateral crura. Cephalic trim should be performed when there is fullness (bulbosity) in the supratip or supraalar region due to protrusion of the cephalic margin of the lateral crura.
The surgeon should leave 7 mm to 9mm of lateral crus. This determination is made on a patient-to-patient basis. The strength of the lateral crura and alar side-walls should be considered. With strong cartilages, more cartilage can be excised, and with weak cartilages, more cartilage should be preserved.
Complete strip is illustrated here via the external rhinoplasty approach but was illustrated earlier in this text via the cartilage-splitting approach (Chapter 5, Figs. 1-3). In a cartilage-splitting approach, the attachments of the lateral crura to the skin/soft-tissue envelope are undisturbed, and a complete strip of 6 mm to R mm should be preserved. Cephalic resection of lateral crux may also be accomplished via the retrograde dissection approach and via the delivery approach.
Minimize lateral resection of the cephalic margin of the lateral cr u r a. Change in tip contour is primarily effected by medial excision, and lateral excision can con-tribute to valve collapse and supraalar pinching.
Thin skin, strong cartilages, and bifidity is a common triad that should be recognized. These patients are at higher risk for bossy formation if excessive cartilage is excised from the cephalic margin of the lateral crura (Appendix G).
Transdomal suture placement can create excessive fullness in the infratip lobule. The infratip lobule should be assessed after transdomal suture placement. Additionally, the lateral aspect of the lateral crura may medialize into the airway with placement of a transdomal suture. If this occurs, it may be necessary to apply lateral crural strut grafts to straighten the lateral crura. On rare occasions, the lateral -most aspects of the lateral crura may need to be trimmed.
Separate dome binding sutures are better able to correct asymmetric domes.
Tip Grafts
Before closure, all edges of the tip graft should be rounded off to prevent visibility of the edges of the graft.
Excessively stiff tip grafts should be crosshatched on the caudal surface to allow cephalic bending and a good double break.
Surgeons tend to make shield grafts too narrow. Most grafts should be approximately 8 nun to 10 min in width at the leading edge. In male patients, the tip grafts are generally wider, and typically measure 10 mm to 12 mm in width at the leading edge.
Most cadaver specimens have thin, atrophic skin, so the tip graft will tend to be more noticeable. indeed, we try to avoid the use of tip grafts in patients with thin skin. Tip grafts are ideal for camouflaging subtle tip asymmetries.
Alar Batten Grafts
Alar batten grafts may be placed via an external rhinoplasty approach or into a precise pocket made through an endonasal incision. This graft is nonanatomic and is typically placed caudal to the lateral crura where there is maximal collapse of the lateral nasal wall and supraalar pinching.
If alar batten grafts are placed too far cephalic, excessive fullness over the middle vault will be noted.
Patients should be told that there will be temporary fullness in the area of the graft. This fullness will typically decrease over a 2- to 3-month period.
For maximal support, the alar batten graft should extend over the bone of the pyriform aperture.
REFERENCES
- Johnson CM, Toriumi DM. Open sTructure rkinoplasty. Philadelphia : WB Saunders, 1990.
- Toriumi DM, Johnson CM. Open structure rhinoplasty: featured technical points and long-term follow-up. Facial Plast Sung Clin North Am 1993;1:1-22.
- Tardy ME. Rhinoplastc: the art and the science. Philadelphia : WB Saunders. 1997.
- Tardy ME, Cheng E. Transdomal suture refinement of the nasal tip. Facial Plast Sti n g 1997;4:317-326.
- Tardy ME, Patt BS, Walter MA. Transdomal suture refinement of the nasal tip: long-term outcomes. Facial Plast .Sung 1989;9:275-284.
- Toriumi DM, Tardy ME. Cartilage suturing techniques for correction of nasal tip deformities. Oper Tech OtolanYngol Head Neck Surg 1995;6:265-273.
- Konior R1, Kridel RWH. Controlled nasal tip positioning via the open rhinoplasty approach. Facial Plast Surg Clin North Ant 1993;1:53-62.
- Simons RL. Vertical dome division in rhinoplasty. Outlarvttgol Clin North Am 1987;20:785-796.
- Kridel RWH, Konior RJ. Controlled nasal tip rotation via the lateral crural overlay technique. Arch Otol Head Neck Surg 1991:117:411-415.
- Toriumi DM, Josen J. Weinberger MS. Tardy ME. Use of alar batten grafts for correction of nasal vale col-lapse. Arch Owl Head Neck Surg 1997;123:802-808.
- Constantian MB. The incompetent external nasal vale: pathophysiology and treatment in primary and secondary rhinoplasty. Plast Reconstr Surg 1994;93:919-933.
- Constantian MB, Clardy RB. The relative importance of septal and nasal valhvlar surgery in correcting air-way obstruction in primary and secondary rhinoplasty. Plast Reconstr Slug 1996;98:38-5