Medial Osteotomies
To perform medial osteotomies, insert the osteotome at the junction between the nasal bone and septum. With the two-tap technique, advance the cutting edge cephalad and fade laterally as the frontal bone is reached (Fig. 1). Control the sharp leading edge of the chisel, as it moves under the skin, with the forefinger of the nondominant hand. This fading me- dial osteotomy avoids the thick frontal bone. Medial osteotomies are usually not necessary in cases in which large dorsal humps are excised, leaving an open-roof deformity.
Lateral Osteotomies And Infracture
[Note: The dissector may wish to mark the site of the proposed osteotomy on the skin be – fore proceeding. Perform the lateral osteotomy on one side, and then reflect the skin/soft-tissue envelope laterally to examine it. Is it in proper position’? Is the periosteum intact, or has it been violated’? Is the mucoperiosteum intact?
After assessing the first lateral osteotomy, the skin of the opposite side may be reflected before the osteotomy. This will allow observation of the osteotomy under direct vision.]
The lateral osteotomies run from the most lateral point of the pyriform aperture to a point medial to the inner canthus of the eye, taking a high to low to high path. In practice, this means a starting point 3 mm to 4 mm above the base of the pyriform aperture and adjacent to the head of the inferior- turbinate. The high-to-low lateral osteotomy preserves a small triangle of bone at the base of the pyriform aperture (Fig. 2). Use a 2-mm (unguarded) or 3-mm (guarded or unguarded) curved or flat osteotome. Use a guarded or unguarded osteotome based on preference.
Make a small incision near the base of the pyriform aperture. Although it is not essential, many surgeons create a short subperiosteal tunnel along the path of the proposed lateral osteotomy. Seat the osteotome on the bone 3 nun to 4 mm above the base of the pyriform aperture, and use a gentle two-tap technique to advance the osteotome gradually. Angle the osteotome in a posterior and cephalic direction initially, and then adjust the os teotome so that the cutting edge travels toward a point medial to the inner canthus of the eye. This creates the typical high-to-low-to-high lateral osteotomy. Control the cutting edge by palpation with the thumb or fingers of the nondominant hand as the osteotome travels toward the inner canthus. When the osteotome approaches the level of the inner canthus, rotate the osteotome clockwise on the patient’s right side and counterclockwise on the left side. This will normally fracture the nasal bone inward creating a controlled backfracture. It may be necessary to complete the fracture with thumb pressure.

Figure 1. Fading medial osteotomies. Place an osteotome flat against the septum with the edge facing laterally. Control the sharp leading edge of the chisel, as it moves under the skin, with the forefinger of the nondominant hand. Avoid the thick frontal bone.
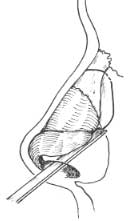
Figure 2. Lateral osteotomies should be started from a point 3 mm to 4 mm above the base of the pyriform aperture to a point adjacent to the inner canthus of the eye. Some rhino plasty surgeons find it helpful to mark the proposed line of the osteotomy on the skin before executing this maneuver.
Intermediate Osteotemies
Chapter 7 – INTERMEDIATE OSTEOTOMIES
An osteotomy between the medial and lateral osteotomies is occasionally indicated. Specific indications include the abnormally contoured nasal bone that is either excessively con – vex or concave. Intermediate osteotomies are most effective for decreasing the curvature of an excessively convex nasal bone. The intermediate osteotomy allows recontouring of the nasal bone for correction of the severely deviated bony vault. This osteotomy is performed before the lateral osteotomy. A 2-mm transcutaneous osteotomy performed midway up the nasal bone is typically used to complete the intermediate osteotomy.
PEARLS
Medial osteotomies are performed to control the backfracture of the nasal bones after lateral osteotomies. If a large dorsal-hump removal was performed, leaving an open roof, it may not be necessary to perform medial osteotomies.
High-to-low-to-high lateral osteotomies are performed to leave a small triangle of bone at the base of the pyriform aperture and prevent medialization of the inferior turbinate.
The dorsal nasal septum at the level of the bony vault must be midline to allow symmetric medialization of the nasal bones. If there is difficulty medializing the nasal bones, a blade handle can be used to shift the bony septum to the midline with the nasal bones.
If a greenstick fracture is noted, a transcutaneous 2-nun osteotome can be used to complete the backfracture and infracture the nasal bone.
Greenstick fractures are acceptable in older patients.
REFERENCES
- Tardy ME. Rhinoplasty : the art and the science. Philadelphia: NVB Saunders, 1997.
- Larrabee NVF Jr. Open rhinoplasty and the upper third of the nose. Facial Plast Sting Clin North Ant 1993:1: 23—28.
- Johnson CM Jr. Toriumi DM. Open structure rlunopla.cq’. Philadelphia: WB Saunders, 1990.
- Murakami CS, Larrabee WF. Comparison of osteotomy techniques in the treatment of nasal fractures. Facial Plctst Sur , 1992;8.209—219.
- Farrior RT. The osteotomy in rhinoplasty. Lca:wt , Go.ccope 1978:88:1449.
- Thomas JR, Griner NR. Renunler DJ. Steps for a safer method of osteotomies in rhinoplasty. Ica-Yngoscope 1987:97:746—747.