Incisions and Approaches
Incisions are methods of gaining access to the bony and cartilaginous structures of the nose and include trans-cartilaginous, inter-cartilaginous, marginal, and trans-columellar incisions. Approaches provide surgical exposure of the nasal structures including the nasal tip and include cartilage-splitting (trans-cartilaginous incision), retrograde (inter-cartilaginous incision with retrograde dissection), delivery approach (inter-cartilaginous, marginal incisions), and external (trans-columellar and marginal incisions). Based on an analysis of the individual patient’s anatomy, appropriate incisions, approaches, and tip-sculpturing techniques are selected (1) (Appendix E).
In this section, a trans-cartilaginous incision is performed on one side. Then an inter-cartilaginous and marginal incision is made on the other side to deliver that cartilage. Next, proceed with the external rhinoplasty approach. Following these instructions will allow an experience with several incisions and approaches in a single specimen.
Delivery Approach
Intercartilaginous Incision
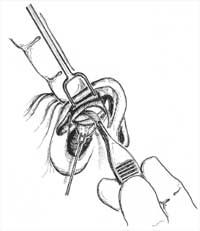
By using a two-prong retractor, evert the caudal margin of the nostril and, by applying pressure with the middle finger of the nondominant hand, reveal the gap between the cau dal margin of the upper lateral and the cephalic margin of the lower lateral cartilages. With a scalpel, make an intercartilaginous incision in this location (Fig. 4) (1,2).
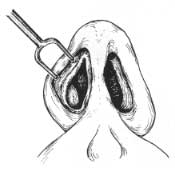

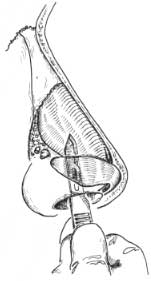
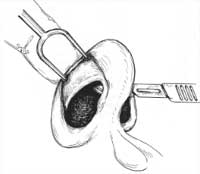

Figure 4. A-C: Intercartilaginous incision. D: For an intercartilaginous approach, bilateral intercartilaginous incisions are connected in the midline over the anterior septal angle, and the incision extends anterior to the caudal septum as a high partial-transfixion incision. Ex posure of the middle and upper nasal vault proceed as described in the text. E: After com pletion of the intercartilaginous approach, a Converse retractor (or other appropriate retrac tor) may be inserted through the incisions, beneath the skin/soft-tissue envelope, to provide exposure of the upper two thirds of the nose.
Marginal Incision
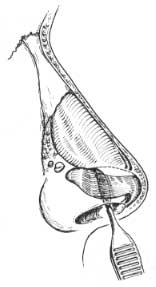
By using a two-prong retractor, evert the caudal margin of the nostril in which an inter-cartilaginous incision was made and, by applying pressure with the middle finger of the nondominant hand, define the caudal margin of the lower lateral cartilage. Pressing cephalad on the nasal dome will cause the caudal margin to appear laterally. Remember that the non-hair-bearing area is a guide to the caudal margin of the lateral crus. Furthermore, pal pation of the cartilage edge with the handle of the scalpel can be helpful before cutting. By using the two-prong retractor to obtain proper exposure, make the marginal incision just caudal to the caudal edge of the lower lateral cartilage (Fig. 5). Great care must be taken as the lateral incision nears the midline. Make sure that the incision follows the cartilage edge and does not take a “short-cut” along the alar rim, which can damage the facet area. Great care must be taken not to cut across a narrow dome or intermediate crux (1,2).


Figure 5. Marginal incision. The nondominant hand is critical to obtain proper exposure.
Delivery of lower lateral cartilages
At this stage, an intercartilaginous incision and marginal incision on one side and a transcartilaginous incision on the other side have been made. Reinsert the two-prong re-tractor into the nostril with the intercartilaginous and marginal incisions and present the caudal margin of the lower lateral cartilage with the aid of pressure from the third finger of the nondominant hand.
Use a slightly curved, fine-pointed dissecting scissors to lift and dissect the soft tissues from the surface of the lower lateral cartilage (Fig. 6). Perform this dissection by inserting scissors into the marginal incision laterally and then separate the perichondrium of the lower lateral from the overlying external skin and soft tissue with a spreading motion. If this is difficult, caudal traction on the vestibular skin underlying the lower lateral cartilage, with a tine two-prong hook, will facilitate this maneuver (Fig. 7) by pulling the lateral crus into the vestibule and thus opening up the potential dissecting plane. Avoid damaging the overlying muscle and nasal vasculature (1,2).

Figure 6. Dissect the soft tissues from the superficial surface of the lower lateral cartilage.
Do not work too far laterally. The lateral one fourth of the lower lateral cartilage should be avoided by the surgeon in nearly all cases.
Place the hook end of a Nievert retractor through the intercartilaginous incision and draw the now-free lateral crus down, like a visor, until it appears outside of the vestibule. It can be held in this position by the Nievert or by another suitable instrument (Fig. 8).
Examine the lower lateral cartilages for unique anatomic features and asymmetries.
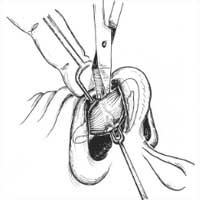
Figure 7. Caudal traction on the vestibular skin underlying the lower lateral cartilage with a fine two-prong hook pulls the lateral crus into the vestibule and opens the potential dissecting plane.
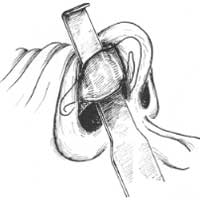
Figure 8. Delivery of lateral crus of lower lateral cartilage.
Transcartilaginous or Cartilage-Splitting Approach
As demonstrated in the accompanying figures, use a two-prong retractor and the middle finger of the nondominant hand to expose the lower lateral cartilage (LLC).
Locate the caudal and cephalic margins of the lateral crura. (The surgeon must identify the cephalically positioned lateral crus when it is present before executing this incision.) Make an incision through vestibular skin only 5 mm to 8 mm cephalic to the caudal 4 margin of the lateral crux of the LLC incision. Figure I illustrates the site of a transcartilaginous incision and the more cephalic location of an intercartilaginous incision. With scissors, dissect free the vestibular skin in a cephalic direction to just beyond the cephalic edge of the lateral crus (Fig. 2). Then incise the lateral crural cartilage and free the cephalic portion (to be removed) from its remaining soft-tissue attachments by dissecting superficial to it in the supraperichondrial plane. Use a skin hook to retract the caudal vestibular skin and another skin hook to retract the nostril margin. An assistant may hold the skin hook that re -tracts the nostril margin, while the surgeon grasps the cartilage to be removed and completes the excision by dividing any last soft-tissue attachments with scissors (Fig. 3) (1,2).
Figure 1. Retraction with a wide two-prong retractor and the middle finger of the nondominant hand exposes the transcartilaginous incision site and also the more cephalically located intercartilaginous incision site.

Figure 2. In a cartilage-splitting approach, dissect the vestibular skin in a cephalic direction to just beyond the cephalic edge of the lateral crus. Then assess how much lateral crus should be removed, and incise the lateral crural cartilage. Be sure to leave ?7 mm to 9 mm of intact strip.
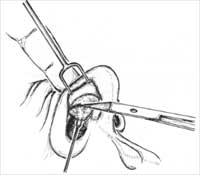
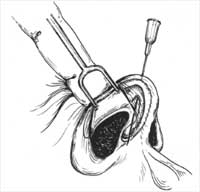
Figure 3. A:
Use a skin hook to re-tract the caudal vestibular skin and the nostril margin. Free the cephalic portion (to be removed) from its remaining soft-tissue attachments by dissecting superficial to it in the supraperichondrial plane. Grasp the cartilage to be removed, and complete the excision by dividing any last soft-tissue attachments with scissors. B: The cartilage incision must come far enough medially to include the cephalic lateral crus at the dome region, or else supratip fullness may persist. However, it is important not to incise too far inferomedially, or the cartilage (which is typically narrow at this region) may be excessively weakened or divided. C: A 30-gauge needle placed percutaneously at the dome can help guide the medial aspect of the transcartilaginous incision in selected cases.