Nasal Dissection: Septoplasty with Cartilage Harvest
Hemitranslixion Incision with Anterior Septal Tunnels
I . Retract the columella with a small nasal speculurn, multitoothed Brown Adson forceps, large two-prong hook, or another suitable instrument. This maneuver exposes the caudal margin of the septum (1,2).
Make a hemitransfixion incision along the caudal border of the cartilaginous septum with a no. 15 blade or no. 15-C blade. In this exercise, a hemitransfixion incision ex- tending from the anterior septal angle to the posterior septal angle is used to gain access to the caudal septum. A Killian incision can be used if access to the caudal septum is not necessary (Fig. IA).
In rare cases, the nasal spine should be exposed.
With a no. 15 blade, small, sharp-pointed scissors, or other suitable instrument, incise the perichondrium of the septum adjacent to the caudal septum on one side.
Perform a subperichondrial dissection along the lower half of the septum to allow har vesting of septa) cartilage. Do not extend this dissection too high, so that later in the dissection a precise pocket tunnel can be made to place a spreader graft via an endonasal approach.
Repeat maneuver 5 on the opposite side of the septum.
If the septum needs any shortening, now may be a good time to perform selective exci sion of the caudal aspect of the septum (Fig. 1 B D). If rotation of the nasal tip is necessary, a superiorly based triangle of caudal septum can be excised (Appendix F). For an obtuse nasolabial angle, the posterior septal angle can be trimmed. For a tension nose deformity (3) or hanging-columella deformity, the entire caudal septum may need to be trimmed. Instead of resection, an overly long midline caudal septum can be sutured between the medial crura to provide support. increase projection, and set tip-rotation and alar colurnellar relation.


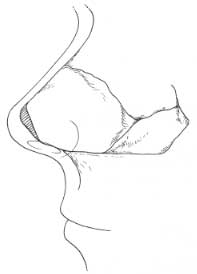
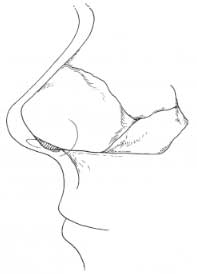
Figure 1. A: A hemitransfixion incision (short dotted lines) or a Killian incision (longer dotted lines) may be used to perform septoplasty. B: Conservative excision in an overlong septum of a thin wedge of caudal septum to decrease columellar show or shorten the nose. C: Excision of a wedge of caudal septum with the base of the excised wedge anterior, for increased rotation. D: Excision of excessive septum at the posterior septal angle to decrease fullness of the nasolabial angle.
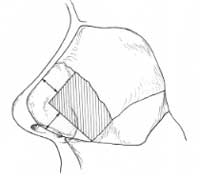
Figure 2. A generous L-strut of -15 mm must be preserved to maintain adequate nasal support. If a dorsal-hump excision is planned, this must also be accounted for in preservation of an adequate L-strut.
Septal Surgery with Harvesting of Cartilage
Carry out a routine septoplasty or submucous-resection operation. To harvest septal car tilage, disarticulate the cartilaginous septum from its bony attachment (osseocartilaginous junction), leaving an ample attachment superiorly (dorsally) at the “Keystone” area. Incise the cartilage dorsally and caudally, preserving ? 15 nun anteriorly to support the nasal tip, and being sure that ? 15 nun will remain dorsally after hump removal (Fig. 2). Preserve this harvested septal cartilage for use as struts or grafts later on in this exercise. If inadequate septal cartilage is available, plan to harvest auricular cartilage for grafting purposes.
Note: We have described septoplasty via a hemitransfixion or a Killian’s incision. A vi – able alternative is to approach the caudal septum directly by performing an external rhino plasty approach and separating the medial crura, thereby coming upon the caudal septum (Fig. 3). Septoplasty may then proceed as described earlier. Although this approach avoids the need for a septal mucosal incision, it is a more complex approach and carries with it a higher risk of loss of tip support if appropriate supportive maneuvers (e.g., columellar strut, caudal extension graft) are not undertaken. This approach is ideal in patients who have an overly long midline caudal septum (tension nose deformity). In these cases, the medial crura can be dropped back and sutured to the midline caudal septum. This maneuver will allow shortening of the nose, deprojection of the nasal tip, or correction of the hanging columella deformity.
PEARLS
Special care must be taken to be sure the dissection is in the subperichondrial plane. If there is any blood-tinged tissue over the surface of the cartilage, there may be a layer of perichondrium left on the cartilage.
To correct a spur along the floor, a subperiosteal tunnel can be dissected along the floor and connected to the dissection above the junction of the septum and maxil lary crest. This method of dissection will minimize the chance of tearing the mucosal flap along the maxillary crest.
If the surgeon plans to apply spreader grafts into precise submucosal tunnels, a bridge of mucosa should be left on the dorsal septum. This will allow the surgeon to create tunnels under the junction of the upper lateral cartilages and septum to accept the grafts.
If the surgeon plans to approach the caudal margin of the septum to correct deformity or to shorten the septum, the septum can be approached through the external rhinoplasty approach.






Figure 3. To perform septorhinoplasty, a viable approach to the septum is to perform an external rhinoplasty approach and separate the medial crura, thereby coming upon the caudal septum, and then proceeding with elevation of mucoperichondrial and mucoperiosteal flaps in standard fashion. Before dissection, local anesthetic should be injected between the medial crura and into the vestibular skin caudal to the caudal septum. While an assistant holds the lower lateral cartilages laterally (A), the surgeon dissects between the medial crura (B) until the caudal septum is identified (C). Special care must be taken to remain in the proper plane between the crura. The mucoperichondrial flaps are next further developed with an elevator (D). The dorsal septum can be divided from the upper lateral cartilages in an anterior-to-posterior direction (E) after both mucoperichondrial flaps have been elevated to the junction of the up-per lateral cartilage and septum (extramucosal dissection). This will allow preservation of continuity of the intranasal mucosa while dividing the upper lateral cartilages from the dorsal septum. Bilateral mucoperichondrial flaps are developed for wide access to the septum (F). Appropriate supportive maneuvers (e.g., columellar strut, caudal extension graft) are undertaken because of the risk of loss of tip sup-port. With an overly long caudal septum, the medial crura can be sutured back on a midline caudal septum to provide support and set tip position.
After dissecting between the medial crura to approach the septum, the medial can be dropped back and sutured to an overly long midline caudal septum. This maneuver will create a more rigid nasal tip without normal tip recoil.
If significant bleeding is noted, the surgeon can re-inject the mucosal flaps and place neurosurgical pledgets bilaterally to compress the mucosal flaps.
REFERENCES
Tardy ME. Rhinoplasty: the art and the science. Philadelphia: WB Saunders, 1997.
Beeson WH. The nasal septum. Otolarvngol Clin North Am 1987;20:743-767.
Johnson CM Jr, Godin MS. The tension nose: open structure rhinoplasty approach. Plastic Reconstruction 1995; 95:43-51.