Rhinoplasty Analysis 1
Development of an operative plan that will achieve the desired outcome requires an under-standing of the patient’s wishes and selection of appropriate surgical maneuvers to effect the proposed changes. The surgeon must be able to identify anatomic constraints that will limit the ability to change contour (thick skin, weak cartilages, etc.). Experience with rhino plasty over time has shown that detailed anatomic analysis of the nose is an essential first step in achieving a successful outcome. Failure to recognize a particular anatomic point preoperatively will often lead to a less than ideal long-term result.
After you have identified the various anatomic landmarks in Chapter 1, undertake a pre-operative rhinoplasty analysis of your patient (cadaver specimen). In this programmatic dissection, you will perform a number of incisions, approaches, and surgical techniques, but it is also important to develop your skills in rhinoplasty analysis. Repeated practice of rhinoplasty-analysis skills will improve your preoperative diagnostic ability. Therefore, in this exercise, determine what the best approach and techniques would be in your specimen. Follow the simplified rhinoplasty-analysis algorithm provided as you examine the face and nose.
Also provided is a more detailed description of terms and a more detailed review of rhinoplasty analysis.
Rhinoplasty Analysis 2
A thorough physical examination and accurate preoperative analysis are critical to achieving the desired long-term postoperative rhinoplasty result. Some degree of mental organization assists in the execution of the physical examination. Visual examination and finger palpation are equally important in the nasal evaluation. Throughout the evaluation, a mental image of the potential outcome and surgical limitations inherent in every individual should be visualized. In effect, the potential rhinoplasty operation is rehearsed even as the physical examination proceeds (1,6).
Study of the standard preoperative photographic images for rhinoplasty (frontal, base, lateral, oblique) allows a systematic, detailed anatomic analysis that complements the phys ical examination process. This chapter focuses on analysis of the four standard rhinoplasty photographic views (frontal, base, lateral, oblique). Emphasis is placed on anatomic descriptions of structures and their relationships to other structures.
Analysis begins by examining all four views and making an assessment of the overall stature of the patient, the facial skin quality, and the symmetry of the face. The principle of dividing the face into horizontal thirds and vertical fifths is it useful tool to obtain a general sense of any incongruent areas of the face that may play a key role in nasal appearance and the outcome of nasal surgery. It is essential that these incongruent areas or asymmetries be recognized and discussed with the patient. Thickness and quality of the facial skin-subcutaneous tissue complex must be determined, as it plays a critical role in dictating the limitations of what can and cannot be accomplished with aesthetic nasal surgery (1,6,7).
After completing the general assessment, note and highlight the most striking characteristics of the nose. These are typically the characteristics that bring the patient for rhino plasty, such as excessive size, deviation, or a dorsal hump. These primary patient concerns must be recognized, highlighted, and addressed above all else.
As the surgeon reviews each photographic image, the major aesthetic and technical points that can be evaluated on a given view are noted first. Subtleties in analysis are then addressed. It is important to recognize both the characteristics of greatest concern to the pa tient and the more subtle findings. The patient may not notice these other subtle abnormal ities if they are left unaddressed by the surgeon. Postoperatively, the scrutinizing patient may notice and point out these abnormalities. Stepwise, methodical analysis of the patient and the photographic views allows the well-trained surgeon to identify significant anatomic and aesthetic points.
Frontal View
On frontal view, the observant surgeon first notes nasal width, any deviation from the midline, and characteristics of the nasal tip. Nasal width can be assessed in the upper, middle, and lower third of the nose. It is important to recognize that a saddle deformity of the bony or cartilaginous dorsum will contribute to the appearance of an overwide dorsum on frontal view, whereas a hump will give the impression of a narrow dorsum. Similarly, a low bony dorsum will create an illusion of a relatively wide upper third of the nose and wide intercanthal distance or pseudohypertelorism (7). This appearance can be significantly im proved by augmenting the nasal dorsum. The width of the nasal base on frontal view should approximate the intercanthal distance.
The contour of the curved aesthetic lines that follow the eyebrows, traverse the radix, and continue down along the lateral nasal dorsum to end at the tip-defining points (the brow-tip aesthetic lines) should be followed, and any asymmetries, twists, or deviations noted. These brow-tip aesthetic lines should be smooth, unbroken, gently curved, and symmetric (1,6).
The nasal tip should be characterized on frontal view with regard to symmetry and definition. Concavity or other anatomic findings of the afar sidewall are noted. Vertical and horizontal aspects of bulbosity should be recognized when present. Bifidity of the nasal tip may be visible on this view (but is typically best appreciated on base view). The gentle “gull-in-flight” relationship of the nasal alae to the infratip lobule should be followed, and any asymmetry should be noted. Exaggeration of this curve is suggestive of alar retraction and/or a dependent infratip lobule. If the columella is not visible (“hidden columella”) on frontal view, this also may indicate a retracted columella. The vertical position and symmetry of the alar insertions should be described on the frontal view.
Base View
On base view, special attention should be given to triangularity, symmetry, columella/lob ule ratio, and width and insertion of the afar base. The nasal base should be configured as an isosceles triangle with a gently rounded apex at the nasal tip and subtle flaring of the afar sidewalls (Fig. 3) (4,8,9). Poor triangularity or trapezoidal configuration with broad domal angles may suggest abnormal divergence of the intermediate crura. The presence of asym metry of the tip may best be appreciated on this view. Often one can visualize the outline of
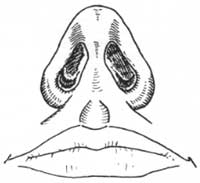
Figure 3. Nasal analysis: Base view. Give special attention to triangularity, symmetry, columellar/lobule ratio, and width and insertion of the alar base.
the lower lateral cartilages beneath the thin skin of the columella and alar rim, and asymmetries or buckling can be noted. Overlong or short medial crura may be apparent: a wide columella and flaring of the medial crural footplates should be noted when present. One should look into the nasal vestibule to identify possible recurvature of the lateral aspect of the lower lateral cartilage (lateral crura), which on occasion contributes to nasal obstruction or correlates with an alar concavity seen on frontal view. This recurvature of the lateral crura can be accentuated with application of dome-binding sutures (transdomal sutures, etc.), resulting in nasal airway obstruction. The caudal septum may be seen protruding into a nostril. Asymmetric nostrils or protruding medial crural footplates may be a clue of subtle caudal septal deviation or asymmetry. Asymmetric orientation of the nostril apices may be indicative of underlying abnormalities of the domal region of the lower lateral cartilages.
The width of the alar base should be noted, with normal width generally being within it vertical line dropped from the medial canthi. Variations in the appearance of width on the base view may be due to the variation in horizontal position of the alar insertions on the face or in the flare of the alar sidewalls. The alar sidewalls themselves are characterized with regard to thickness and flare. Alar base insertions are described by degree of recurva ture. with straight insertions going directly into the face (i.e., no nostril sill), and extremely recurved alae inserting directly into the columella (4,8,9).
The ratio of the columella to lobule should approximate a 2:1 ratio, and the beginning of the flare of the medial crural footplates should divide the alar base into halves. The nostrils are commonly oriented 30 to 45 degrees toward the midline and are pear-shaped and elongated. The facets or external soft-tissue triangles are attractive when they are well defined but can detract if they are overly conspicuous (4,8,9).
Lateral View
The lateral view offers important information on tip projection, nasal length, dorsal profile, and alar-columellar relationship.
The nasal tip should ideally project strongly from the face and gracefully lead the supratip dorsum, creating a modest supratip break. An identifiable but not overly exaggerated columellar double break typically marks the junction of the medial and intermediate crux. Nasal tip projection is consistently assessed by using the method described by Goode (see Fig. 2) (2,3). If the length of a line drawn from the tip-defining point perpendicular to a tangent to the alar-facial junction is greater than 0.55 to 0.60 of the line drawn from the nasion to lip-defining point, then the nose may be over projected. However, when assessing tip projection, relationships between the nose and other aesthetic facial features (chin projection, forehead contour, ethnic background, etc.) must be considered.
Nasal length is complicated to define. The nasal length is compared with the horizontal thirds of the face and the overall stature of the patient to determine whether the nose is of appropriate length. However, the factors contributing to the appearance of nasal length are complex. The nose can be considered to have three lengths, with nasion to tip being the cen tral length, and nasion to alar margin being the lateral lengths. A short or long lateral length may reflect a retracted or hooded ala, respectively, whereas a short or long central length may reflect an obtuse or acute nasolabial (columellar-labial) angle, respectively. Further-more, a deep nasofrontal angle contributes to the illusion of a short nose, and a shallow nasofrontal angle adds apparent length to the nose (10). In Fig. 4A, three diagrams identical except for the nasofrontal angle illustrate the effect of the nasofrontal angle on the appearance of nasal length. Another three diagrams (Fig. 413), identical except for the nasolabial angle, illustrate the effect of the nasolabial angle on the appearance of length.
The nature of the columellar-labial confluence and columellar-lobular angle (double break) also must be assessed. Webbing or tenting of the columellar-labial confluence should be noted. An overly obtuse columellar-labial angle and/or an exaggerated double break will make the nose appear short, whereas the converse (acute columellar-labial angle and/or absent double break) will add apparent length. A posteriorly inclining lip or deficiency of the premaxilla may confound accurate measurement of the columellar-labial
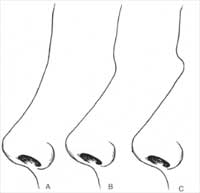
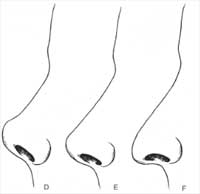
Figure 4. A deep nasofrontal angle and/or an obtuse nasolabial angle contributes to the appearance of a short nose, whereas a shallow nasofrontal angle and/or an acute nasolabial angle adds apparent length. In the first three line drawings (A), the nasolabial angle is the same, whereas the nasofrontal angle is altered to illustrate the effect of the nasofrontal an gle on the appearance of nasal length. In the next three drawings (B), the nasofrontal angle is constant, whereas the nasolabial angle varies.
angle. The relationship of the nose to other facial structures also will influence nasal length;
for example, a flat forehead will give the illusion of increased nasal length (10).
Byrd (5) described a useful method for determining appropriate aesthetic proportions for tip projection, nasal length, and radix projection. “Ideal” nasal length is two thirds of the midfacial height and is equal to chin vertical. Tip projection is ideally two thirds of this planned or ideal nasal length. Radix projection may be measured from the junction of the nasal bones with the orbit and ideally should be one third of the calculated nasal length.
Byrd recommended the plane of the cornea surface as a preferred reference point for radix projection; from this starting point, the radix projects 0.28 times the ideal nasal length. In Byrd’s report, the radix projected 9 to 14 mm from the plane of the cornea surface (5).
One should be familiar with the aesthetic angles applied in facial analysis as general guidelines for standards of facial aesthetics and facial harmony. Powell and Humphries aesthetic triangle (nasofacial, nasofrontal, nasomental, and mentocervical angles) and the nasolabial angle or confluence are a few of the more commonly cited measurements (3).
Assessment of the dorsal contour should identify any concavity, convexity, or irregularity. A high dorsum with a slight concavity at the rhinion is generally considered the aesthetic ideal in the white female nose. A high dorsum that is straight or with a small hump is ideal in a white male nose. Other notable components of the dorsum include the nasal starting point, which is ideally positioned at the level of the superior palpebral fold, and the tip-supratip relationship, as previously mentioned.
The ala is analyzed in detail on the lateral view. Insertion of the ala on the face 2 to 3 nun above the columella in the horizontal plane, as described by Crumley (4), is judged to be normal. The contour of the alar rim in profile ideally approximates a “lazy S” shape: one should note if this is normal, exaggerated, or straight. The size of the alar lobule is classified as small, normal, or large. The alar-columellar relationship should be precisely de- scribed. The range of normal columellar show is generally considered to be 2 to 4 nun. The complexities of the alar-columellar relationship were categorized by Gunter et al. 01), who identified abnormal positioning of the ala and the columella in relationship to a line drawn through the long axis of the nostril. All patients have it hanging, normal, or retracted ala and a hanging, normal, or retracted colurella. Thus nine possible anatomic combinations make up the alar-columellar relationship (Fig. 5).
On lateral view, the long axis of the nostril should rise at approximately 10 to 30 degrees from a plane horizontal to the Frankfurt plane. This is a reliable determinant of the need for operative rotation of the nasal tip (7).
Oblique View
Although it offers the least amount of objective data, this is an important aesthetic view be – cause the nose is most often seen at oblique angles. Several aspects of nasal contour are high – lighted on this view and should be assessed. The brow-tip aesthetic lines and the soft-tissue facets are especially prominent and should he carefully assessed, as irregularities may be highlighted on this view. Furthermore, abnormalities of the lateral aspect of the nasal bones, nasal length, dorsal height, and tip projection also may be highlighted on the oblique view.
Overview
There is no “standard” rhinoplasty. Each operation is unique in that it must be tailored to the specific anatomic components involved and the desires of the patient. By developing a consistent, meticulous routine in which the patient’s nose is analyzed with regard to its anatomic components and their complex inter r elationships, the surgeon can select the best incisions, approaches, and techniques to achieve the desired surgical outcome.
PEARLS
The soft-tissue point correlating to the osseocartilaginous junction of the nasal dorsum is the rhinion. The skin at this location is relatively thin compared with the thicker skin of the nasion. This is important to recognize when planning dorsal-hump reduction. After hump reduction, this area must be very smooth to avoid visible or palpable irregularities (see Appendix G).
The nasal starting point typically cor r esponds to the nasion. in female patients, it is ideally situated at the same level as the superior palpebral fold.

Figure 5. Nine possible anatomic combinations making up the alar-columellar relation-ship.
The nasal tip should be the most anteriorly projecting portion of the nose. The nasal tip should ideally lead the supratip dorsum, creating a modest supratip break.
A “pollybeak” is a postoperative situation in which the supratip leads the tip. Causes for a pollybeak include underresection of cartilaginous dorsum at the ante rior septal angle, excessive scar tissue formation, and inadequate support of the tip, causing postoperative loss of tip projection.
An identifiable but not overly exaggerated columellar double break usually marks the junction of the medial and intermediate crus.
Nasal-tip projection may be consistently assessed by using the method described by Goode. if the length of a line drawn from the tip-defining point perpendicular to a tangent to the alar-facial junction is greater than 0.55 to 0.60 of the line drawn from the nasion to tip-defining point, then the nose may appear overprojected.
Thickness and quality of the facial skin-subcutaneous tissue complex must be determined, as it plays a critical role in dictating the limitations of what can and can-not be accomplished with nasal surgery.
Thin skin, strong cartilages, and bifidity: an important anatomic triad. The surgeon must recognize the need to approximate the tip-defining points to improve tip tri angularity. The surgeon must recognize the risk of bossa formation if excessive lat eral crura is excised (see Appendix G).
Facial analysis can describe vertical facial thirds: trichion-to–label la, glabella-to subnasale, and subnasale-to-menton. However, the hairline is variable, and at times the glabella is not always precisely identifiable. Another method considers the lower two thirds of the face from the nasion to the menton. The nasion-to-subnasale distance is 47% of the total, whereas subnasale to menton is 53% (Fig. 6).
The astute surgeon will be able to anticipate the contour of the lower lateral cartilages by studying surface topography of the nasal tip.
The basal view provides information about the shape of the lower lateral cartilages. A trapezoidal nasal base indicates a wide domal angle and indicates the need for a tip technique that will create a more acute dome angle (done-binding suture, etc.).
Cephalic positioning of the lateral crura is indicated by the “parenthesis” deformity and lack of lateral wall support.
The “narrow nose syndrome” is noted in patients with a projecting nose, short nasal bones, and long upper lateral cartilages. These patients are at high risk for inferome dial collapse of the upper lateral cartilages after dorsal-hump excision. These patients frequently need spreader grafts. The contour of the caudal margin of the medial and intermediate crura can frequently be assessed by close examination of the nasal base.
ILLUSIONS IN RHINOPLASTY
A dorsal convexity or hump frequently gives the appearance of narrowness on frontal view. It also provides the illusion of relative decreased projection. That is, changing the relationship between the dorsum and tip can improve the appearance of projection.
A low dorsum gives the appearance of increased nasal width due to less shadowing along the lateral nasal wall.
A saddle deformity of the bony or cartilaginous dorsum will contribute to the appearance of an overwide dorsum on frontal view, whereas a hump will give the impression of a narrow dorsum. Similarly, a low dorsum will create an illusion of a relatively wide upper third of the nose or pseudohypertelorism. This appearance can be significantly altered by augmenting the nasal dorsum.
A deep nasofrontal angle lends the appearance of a short nose, as does an obtuse nasolabial angle or an accentuated double break.

Figure 6. Relationship of the lower two-thirds of the face.
REFERENCES
I . ‘Lardy ME. Rhinoplasty: the art and the science. Philadelphia: WB Saunders, 1997.
Tardy ME, Walter MA, Pau BS. The overprojecting nose. anatomic component analysis and repair. Facial Plastic Surgery 1993;9:306-316.
Ridley MB. Aesthetic facial proportions. In: Papel ID, Nachlas NE, eds. Facial plastic and reconstructive staWerv. Philadelphia: Mosby Year Book, 1992:99-109.
Crumley RL, Lanser M. Quantitative analysis of nasal tip projection. Larvrtgoscope 1998;98:202-208.
Byrd HS, Hobar PC. Rhinoplasty: a practical guide for surgical planning. Plastic Reconsir Surgery 1993;91: 642-656.
Tardy ME, Brown R. Surgical anatomy of the nose. New York: Raven Press, 1990.
Johnson CM, Toriurni DM. Open structure Rhinoplasty. Philadelphia: Saunders, 1990.
Tardy ME. Patt BS. Walter MA. Alar reduction and sculpture: anatomic concepts. Facial Plastic Surgery 1993;9: 295-305.
Becker DG, Weinberger MS. Greene BA, Tardy ME. Clinical study of alar anatomy and surgery of the alar base. Arch Otolaryngology Head Neck .Stag 1997;123:789-795.
Tardy ME, Becker DG. Weinberger MS. Illusions in rhinoplasty. Facial Plastic Stag 1995;1 1:1 17-138.
Gunter JP, Rohrich RJ, Friedman RM. Classification and correction of alar-columellar discrepancies in rhinoplasty. Plastic Reconstructive Surgery 1996;97:643-648.
Surface Angles, Planes, And Measurements
Facial thirds
Upper third: Trichion to glabella
Middle third: Glabella to subnasale
Lower third: Subnasale to menton (Fig. 2A)
Horizontal fifths: Five equally divided vertical segments of the face (Fig. 2B)
Frankfort plane: Plane defined by a line from the most superior point of auditory canal to most inferior point of infraorbital rim (Fig. 2C)
Nasofrontal angle: Angle defined by glabel la-to-nasion line intersecting with nasion-to-tip line. Normal, 115 to 130 degrees (within this range, more-obtuse angle more favorable in female, and more acute angle in male patients; Fig. 2D)
Nasofacial angle: Angle defined by glabella-to-pogonion line intersecting with nasion-to-tip line. Normal, 30 to 40 degrees (Fig. 2E)
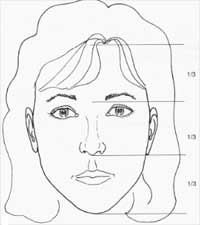
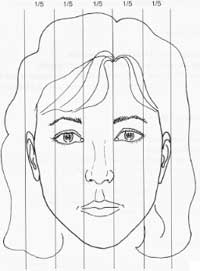
Figure 2. Surface angles, planes, and measurements.
A: Horizontal facial thirds. B: Vertical facial fifths
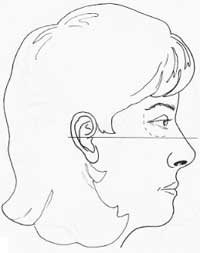
Figure 2, continued. C: Frankfort plane. D: Nasofrontal angle.
Figure 2, continued. E: Nasofacial angle. F: Nasomental angle.


Figure 2, continued. G: Relationship of lips to subnasale-to-pogonion line . H: Relationship of lips to nasomental line .


Figure 2, continued. I: Mentocervical angle . J: Legan’s angle of facial convexity .


Figure 2, continued. K: Nasolabial angle. L: Nasal projection: method of Goode.
PEARIL
Normal projection with a “3-4-5” triangle described by Crumley (see later) gives a nasofacial angle of 36 degrees.
Nasomental angle: Angle defined by nasion-to-tip line intersecting with tip-to-pogonion line. Normal, 120 to 132 degrees (Fig. 2F)
Relationship of lips
To nasomental line: Upper lip, 4 mm behind; lower lip, 2 min behind line from nasal tip to menton (Fig. 2H)
To subnasale-to-pogonion line: Upper lip, 3.5 nun anterior; lower lip, 2.2 mm anterior (Fig. 2G)
Mentocervical angle: Angle defined by glabella-to-pogonion line intersecting with menton-to-cervical point line (Fig. 2I)
Legan facial-convexity angle: Angle defined by glabella-to-subnasale line intersecting with subnasale-to-pogonion line; normal, 8 to 16 degree (Fig. 2J)
PEARL
Useful in assessing chin deficiency, candidacy for chin implant, chin advancement, or other chin alteration
Nasolabial angle: Angle defined by columellar point-to-subnasale line intersecting with
subnasale-to-labrale superius line; normal, 90 to 120 degrees (within this range, more
obtuse angle more favorable in female, and more acute in male patients; Fig. 2K) Columellar show: Alar-columellar relationship as noted on profile view; 2 to 4 mm of columellar show is normal
Nasal projection: Anterior protrusion of nasal tip from face (Fig. 2L)
Goode’s method: A line is drawn through the alar crease, perpendicular to the Frankfurt plane. The length of a horizontal line drawn from the nasal tip to the alar line (alar point-to-nasal tip line) divided by the length of the nasion-to-nasal tip line. Normal, 0.55 to 0.60 (2,3)
Crumley’s method: The nose with normal projection forms a 3-4-5 triangle (i.e., alar point-to-nasal tip line (3), alar point-to-nasion line (4), nasion-to-nasal tip line (5)] (4).
Byrd’s method: Tip projection is two-thirds (0.67) the planned postoperative (or the ideal) nasal length. Ideal nasal length in this approach is two-thirds (0.67) the midfacial height (5)
POWELL AND HUMPHRIES “AESTHETIC TRIANGLE”
Nasofrontal: 115 to 130 degrees Nasofacial: 30 to 40 degrees Nasomental: 120 to 132 degrees Mentocervical: 80 to 95 degrees (3)
Landmarks For Analysis
Points
Trichion: Anterior hairline in the midline
Glabella: Most prominent midline point of forehead, well appreciated on lateral view Nasion: Most posterior midline point of forehead, typically corresponds to nasofrontal suture
Rhinion: Soft-tissue correlate of osseocartilaginous junction of nasal dorsum Sellion: Osseocartilaginous junction of nasal dorsum
Supratip: Point cephalic to the tip
Tip: Ideally, most anteriorly projected aspect of the nose
Subnasale: Junction of columella and upper lip
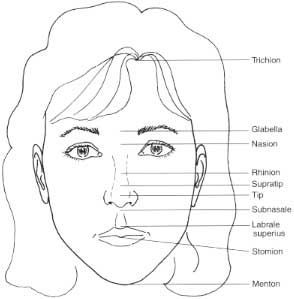
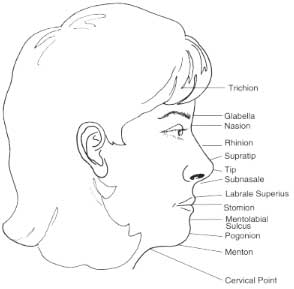

Figure 1. Nasal analysis: Landmarks.
Labrale superius: Border of upper lip
Stomion: Central portion of interglacial gap
Stomion superius: Lowest point of upper-lip vermilion
Stomion inferiors: Highest point of lower-lip vermilion
Mentolabial sulks: Most posterior midline point between lower lip and chin Pogonion: Most anterior midline soft-tissue point of chin
Menton: Most inferior point on chin
Cervical point: Point of intersection between line tangent to neck and line tangent to sub-mental region
Nation: Point of intersection between line from subnasale to pogonion and line from cervical point to menton
Lab Exercise: Nasal Analysis
General
Skin quality: Thin, medium, or thick
Primary descriptor (i.e., why is the patient here): For example, “big,” “twisted,” “large hump”
Frontal View
Twisted or straight: Follow brow-tip aesthetic lines Width: Narrow, wide, normal, “wide-narrow-wide” Tip: Deviated, bulbous, asymmetric, amorphous, other
Base View
Triangularity.: Good versus trapezoidal
Tip: Deviated, wide, bulbous, bifid, asymmetric
Base: Wide, narrow, or normal. Inspect for caudal septal deflection
Columella: Colurnellar/lobule ratio (normal is 2:1 ratio); status of medial crural footplates.
Lateral View
Nasofrontal angle: Shallow or deep Nasal starting point: High or low
Dorsun: Straight, concavity, or convexity, bony, bony-cartilaginous, or cartilaginous (i.e.,
is convexity primarily bony, cartilaginous, or both)
Nasal length: Normal, short, long
Tip projection: Normal, decreased, or increased
Alar-columellar relationship: Normal or abnormal
Naso-labial angle: Obtuse or acute
Oblique View
Does it add anything, or does it confirm the other views?
Many other points of analysis can be made on each view, but these are some of the vital points of commentary