Plumping Grafts
Plumping grafts may he used to open up an acute nasolabial angle, improve a retracted columella, and support a deficient nasal base. Dissect a midcolumellar precise pocket to just above the nasal spine. Place multiple small pieces of cartilage (I mm to 2 mm), harvested from the septum or ear, in the pocket. These grafts will augment the deficient area (Fig. 1) (1,2). Plumping grafts placed below the medial crural footplates will increase sup-port of the nasal base (Appendix F)
Figure 1. Plumping grafts may improve a retracted columella.
Caudal Extension Grafts
Caudal extension grafts have been described for use in correcting a retracted columella, over-rotated tip, short nose, or to increase tip support and projection (3) (Appendix F). This graft is sutured to the caudal margin of the nasal septum and is secured between the medial crura in the midline with 5-0 buried polydioxanone suture (PDS) (Fig. 2). When suturing the caudal extension graft to the caudal septum, the caudal margin of the graft must be in the precise midline. Deviation off the midline will result in a deviation of the nasal base or tip. It is critical to assess nasal projection, length, tip rotation, and alar/columellar relation when positioning a caudal extension graft. Patients should be told preoperatively that their nasal tip will be stiffer, with loss of the normal tip recoil.
Deviated Caudal Septum
A number of maneuvers are at the surgeon’s disposal in the treatment of a caudal septal deviation (4,5). Traditional approaches include scoring the septal cartilage on the concave side, thereby relaxing the “spring” of the cartilage. This may be done as a solitary maneu ver, or in conjunction with a so-called “swinging door maneuver.” As illustrated in Fig. 3, a wedge of cartilage excised along the maxillary crest releases the caudal septal attach ments and allows the septum to swing to the midline. The midline position may be secured with a 4-0 PDS attached to the periosteum adjacent to the opposite side of the nasal spine.
Ethmoid bone splinting grafts or sandwich grafts also may be of benefit in this situation (6). A straight piece of bone is harvested; a large straight Keith needle may be used as a delicate hand-held drill to make holes in the bone graft. The deviated portion of cartilaginous septum may be addressed by scoring on the concave side, and the bone graft or grafts may then be used to splint the septum in a straighter orientation. However, use of the ethmoidbone graft in this location thickens the caudal septum and can contribute to nasal obstruction. The ethmoid bone sandwich grafts may be used to address a deviation of the dorsal septum, where the additional septal thickness caused by this graft is well tolerated (Fig. 4).
In cases of a severely deviated caudal and dorsal septum, the offending portion may be excised and replaced with a straight piece of cartilage, typically harvested from the septum more posteriorly (Fig. 5) (4). Suture fixation to a stable segment of cartilage attached at the osseocartilaginous junction and nasal spine will allow reconstruction of an intact L-strut to support the lower third of the nose. The reconstructed caudal segments can be sutured between the medial crura to set nasal length, projection, rotation, and the alar/columellar relation.
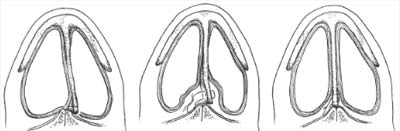

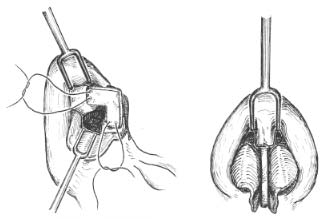


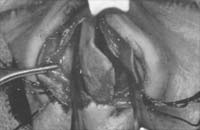
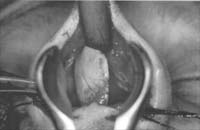

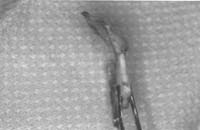
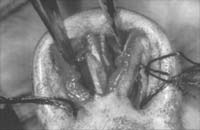


Figure 5. Septal replacement for severe cases of deviated caudal and dorsal septum. In the first case example, a segment of caudal septum is removed and replaced with a straight piece of septal cartilage harvested posteriorly. As illustrated, the replacement cartilage is extended caudally and se-cured between the medial crura as well. In this case, a tip graft also was applied. Preoperative and postoperative comparison. This series of intraoperative photographs illustrates total replacement of the severely deviated caudal septum. The severely deviated component is removed, along with posterior septum. The deviated septum is replaced with straight septal cartilage harvested posteriorly. A tip graft also was applied.
Rib Cartilage Graft Reconstruction of Saddle Deformity
The severe saddle-nose deformity may be treated by using autogenous rib cartilage (8,9).
Harvest of rib is described later. The rib graft is carved into a dorsal graft and a columellar strut, which are interdigitated to recreate an intact L-strut (Fig. 6). This type of structural re-construction is particularly useful when there is complete loss of septal support. If an intact nasal septal L-strut is present, onlay dorsal grafting will be sufficient to correct the deformity. Great care must be taken to adhere to the principle of “balanced cross-sectional carving” to minimize the risk of graft warping. Once in position, the domes can be sutured over the graft with a transdomal suture. An external rhinoplasty approach allows exposure for facile placement of these grafts. A tip graft allows improved tip projection and definition.
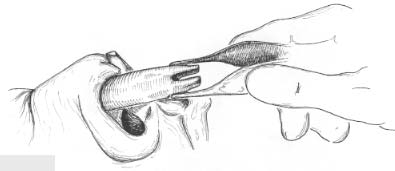

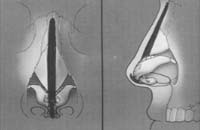













Figure 6. A, B: Severe saddle-nose deformity. Rib graft is fashioned into a columellar strut (secured to the medial crura) and a dorsal onlay graft that interdigitates with the columellar strut. Preoperative (C-F) photographs of a patient with a severe saddle-nose deformity. She underwent application of an iliac bone graft to her nasal dorsum in the past. Lack of an intact L-strut and in-adequate middle vault support resulted in descent of the graft, airway obstruction, and referral to our office for re-construction. Base view reveals the bone graft in the left nostril and a widened columellar scar. Graphic operative worksheet (G, H) illustrates the surgical high points. Rib graft was harvested (I, J), and exposure was achieved via the external rhinoplasty approach (K, L). A sutured-inplace columellar strut fashioned from rib graft was secured between the medial crura (M, N). A dorsal-on lay graft was carefully carved (0, P) with a notch, allowing it to interdigitate with the columellar strut. The dorsal graft was placed and se- cured (Q-T). Example from another patient illustrating interdigitation of strut and dorsal on lay graft (U). A tip graft was placed and covered with a layer of perichondrium to camouflage and soften the leading edge of the tip graft. (V, W).
PEARLS
When placing plumping grafts, the surgeon should overcorrect because the grafts tend to settle over time. Additionally, the pocket can be gently irrigated with antibiotic solution to minimize the incidence of infection.
When performing a caudal extension graft, the surgeon must take special care to set appropriate tip projection, rotation, length, and alar/columellar relation. Additionally, the caudal margin of the graft must be in the precise midline.
The inferior border of the caudal extension graft should be stabilized on the posterior septal angle, soft tissue, or other supporting tissues to avoid postoperative counterrotation of the extension graft.
Deviations of the caudal septum can usually be corrected by crosshatching the cartilage and other conservative maneuvers described in the text. Many cases can be corrected by accounting for excessive length of the L-strut. In rare cases, subtotal septal replacement may be necessary.
When using an integrated columellar strut/dorsal graft, the surgeon must take special care to stabilize the columellar strut in the midline to avoid shifting or tilting of the columella. Placement of the dorsal graft into a precise dorsal pocket or suture fixation of the dorsal graft to the middle nasal vault will minimize the chance of the graft shifting to one side.
Symmetric carving of the costal cartilage graft will minimize the chance of the graft warping over time.
REFERENCES
- Tardy ME, Becker DG, Weinberger MS. Illusions in rhinoplasty. Facial Mast Sure 1995:1 1:117-138.
- Tardy ME. Rhinoplasty: the art and the science. Philadelphia: WB Saunders, 1997.
- Toriumi DM. Caudal septal extension graft for correction of the retracted columella. Oper Tech Otolarvngol Head Neck Surg 1995;6:311-318.
- Beeson WH. The nasal septum. Otolarvngol Clin North Am 1987 : 20:743-767.
- Toriumi DM, Ries WR. Innovative surgical management of the crooked nose. Facial Plast Sti n g Clin North Am 1993;1:63-78.
- Metzinger SE, Boyce RG, Rigby PL, Joseph JJ, Anderson JR. Ethmoid hone sandwich grafting for caudal septal defects. Arch Otolarvngal Head Neck Surg 1994;120:1121-1125.
- Toriumi DM. Subtotal reconstruction of the nasal septum: a preliminary report. Laryngoscope 1994;104: 906-913.
- Daniel RK. Rhinoplasty and rib grafts: evolving a flexible operative technique. Plast Reconstr Stag 1992:94: 597-611.
- Wang TD. Aesthetic structural nasal augmentation. Oper Tech Otolar rngol Head Neck Surg 1990.