Alar Base Resection
Follow the accompanying figures and text to perform alar base resections (1,2).
The site of incisions and the amount, degree, and geometry of alar reductions depend on a host of anatomic variations predetermined before and during surgery. Although the surgeon’s aesthetic judgment will ultimately determine the site and degree of resection, a more precise surgical approach may be determined if several anatomic guidelines are assessed and integrated. Conservatism is mandatory to avoid over-reduction and asymmetry, conditions that are difficult to correct satisfactorily.
As the need for reduction increases, both the incision and excision become more extensive. Alar reduction is a compromise operation, in which greater reductions exact the penalty of a larger scar. The surgeon must balance this compromise with experienced aesthetic judgment and proven scar-camouflage techniques.
Skin sutures placed across the alar-facial junction often lead to permanent suture marks. Effective camouflage at the alar-facial junction may be facilitated by positioning incisions 1 mm to 2 mm above the alar-facial junction. Skin closure can he performed with a cyanoacrylate adhesive (octyl-2-cyanoacrylate, Dermabond; Ethicon, Somerville, NJ, U.S.A.).
Internal Nostril Floor Reduction
In patients requiring minimal alar reduction, excision of a wedge of epithelium and soft tissue from the nostril floor only (Fig. 1) will slightly reduce the alar flare by reducing the dimension of the internal (medial) border. Although the outward curve of the ala is altered, no medial repositioning of the alar-facial junction is effected. The scar is effectively hid – den within the nostril floor if the nostril sill is not violated. At times, the shape of the nostril sill will determine whether this approach is appropriate. Subtle, conservative, but effective improvements are possible with this approach. The dimension of the lateral alar border remains unchanged.
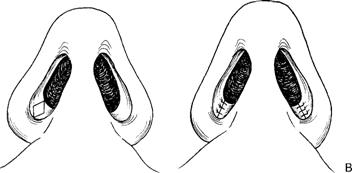
Figure 1. Internal nostril floor reduction will slightly reduce alar flare. WEDGE EXCISION OF NOSTRIL FLOOR AND SILL
Further reduction of alar flare is accomplished by carrying the incision across the sill into the alar facial junction 1 mm to 2 mm above the alar facial crease. Reduction of flare as well as slight reduction of the alar hulk is effected (Fig. 2).
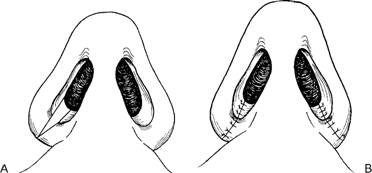
Figure 2. Wedge excision of nostril floor and sill conservatively reduces flare as well as alar bulk.
Alar Wedge Excision
If the alar development is excessive and bulbous, excision of a wedge of ala at the alar-facial junction 1 mm to 2 mm above the alar-facial crease will reduce the overall bulkiness of the alar anatomy (Fig. 3). Some medial repositioning of the alae may be effected with this maneuver. Reduction of the overall length of the alar sidewalls occurs when generous wedges are excised, ideal in the reduction of the alar flare created when correcting the overprojecting tip.
Figure 3. Excision of a wedge of ala at the alar-facial junction 1 mm to 2 mm above the alar-facial crease will reduce the overall bulkiness of the alar anatomy. Some medial repositioning of the alae may be effected with this maneuver.
Sliding Alar Flap
More substantial alar reduction with medial repositioning is effected with a generous incision above the alar-facial junction with various degrees of alar excision (Fig. 4). Reduction of the volume, curve, and flare of both the internal and external alar margins will re sult from this procedure, the extent of each dependent on the angulation of the alar incision. A back cut placed 2 mm above the alar-facial junction allows the alar flap to slide medially, narrowing the alar base significantly.
Figure 4. Sliding alar flap typically incorporates a back cut to allow the alar sidewall to advance medially.
PEARLS
When performing alar base reduction, the surgeon should err on under-correcting the deformity to prevent resection of excessive tissue. Once too much tissue is excised, it is very difficult to correct; be particularly conservative in male patients.
Internal alar base excision can significantly decrease the internal diameter of the nostril and should be performed in a conservative manner. When performed, usu ally 2 mm of tissue is removed.
If an incision is made on the lateral surface of the ala, the incision should be made above the alar crease to minimize scarring. A cyanoacrylate adhesive (Dermabond; Ethicon, Somerville, NJ, U.S.A.) can be used to close the lateral alar incision.
In the incision, the skin edges can be favorably beveled to maximize skin-edge eversion and avoid a depressed scar.
REFERENCES
- Tardy ME, Patt BS, Walter MA. Alar reduction and sculpture: anatomic concepts. Facia/ P/a.rl Surg 1993:9: 295-305.
- Becker DG, Weinberger MS, Greene BA. Tardy ME. Clinical study of alar anatomy and surgery of the alar base. Arch Ofolaryngol Head Neck Surg 1997;123:789-795.