Although the anatomy of the nose has been fundamentally understood for many years, only relatively recently has there been an increased understanding of the long-term effects of surgical changes on the function and appearance of the nose. A detailed understanding of nasal anatomy is critical for successful rhinoplasty. This chapter reviews the surface and structural anatomy of the nose. with an emphasis on important surgical anatomy.
Accurate assessment of the anatomic variations presented by a patient allows the surgeon to develop a rational and realistic surgical plan. Furthermore. recognizing variant or aberrant anatomy is critical to preventing functional compromise or untoward aesthetic results. This chapter presents a limited diagrammatic overview of nasal anatomy. More detailed study of nasal and facial anatomy is recommended (1) (Figs. 1-10).
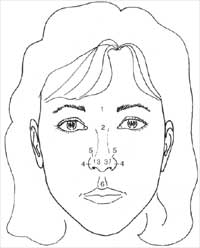
Figure 1. Surface anatomy of the nose: Frontal view. 1, Glabella; 2, nasion; 3, tip-defining points; 4, alar-sidewall; 5, supraalar crease; 6, philtrum.
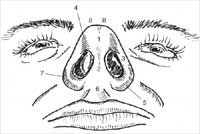
Figure 2. Surface anatomy of the nose: Base. 1, Infratip lobule; 2, columella; 3, alar sidewall; 4, facet or soft-tissue triangle; 5, nostril sill; 6, columella-labial angle or junction; 7, alar-facial groove or junction; 8, tip-defining points.

Figure 3. Surface anatomy of the nose: Lateral. 1, Glabella; 2, nasion, nasofrontal angle; 3, rhinion (osseocartilaginous junction); 4, supratip; 5, tip-defining points; 6, infratip lobule; 7, columella; 8, columella-labial angle or junction; 9, alar-facial groove or junction.

Figure 4. Surface anatomy of the nose: Oblique. 1, Glabella; 2, nasion, nasofrontal angle; 3, rhinion; 4, alar sidewall; 5, alar-facial groove or junction; 6, supratip; 7, tip-defining points; 8, philtrum.
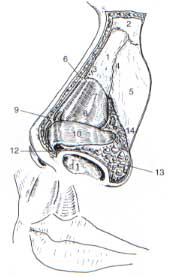
Figure 5. Nasal anatomy: Oblique. 1, Nasal bone; 2, nasion (nasofrontal suture line); 3, internasal suture line; 4, nasomaxillary suture line; 5, ascending process of maxilla; 6, rhinion (osseocartilaginous junction); 7, upper lateral cartilage; 8, caudal edge of upper lateral cartilage; 9, anterior septal angle; 10, lower lateral cartilage, lateral crus; 11, medial crural footplate; 12, intermediate crus; 13, sesamoid cartilage; 14, pyriform aperture.
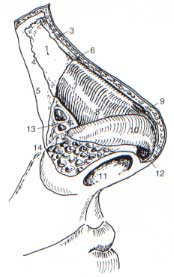
Figure 6. Nasal anatomy: Lateral (rotated slightly obliquely). 1, Nasal bone; 2, nasion (nasofrontal suture line); 3, inter-nasal suture line; 4, nasomaxillary suture line; 5, ascending process of maxilla; 6, rhinion (osseocartilaginous junction); 7, upper lateral cartilage; 8, caudal edge of upper lateral cartilage; 9, anterior septal angle; 10, lower lateral cartilage, lateral crus; 11, medial crural footplate; 12, intermediate crus; 13, sesamoid cartilage; 14, pyriform aperture.
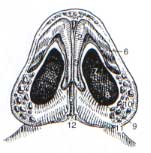
Figure 7. Nasal anatomy: Base. 1, Tip-defining point; 2, intermediate crus; 3, medial crus; 4, medial crural footplate; 5, caudal septum; 6, lateral crus; 7, naris; 8, nostril floor; 9, nostril sill; 10, alar lobule; 11, alar-facial groove or junction; 12, nasal spine.
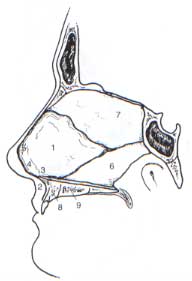
Figure 8. Nasal septum. 1, Quadrangular cartilage; 2, nasal spine; 3, posterior septal angle; 4, middle septal angle; 5, anterior septal angle; 6, vomer; 7, perpendicular plate of ethmoid bone; 8, maxillary crest, maxillary component; 9, maxillary crest, palatine component.
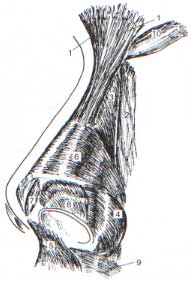
Figure 9. Nasal musculature. A: Elevator muscles: 1, procerus; 2, levator labii alaequae nasi; 3, anomalous nasi. B: Depressor muscles: 4, alar nasalis; 5, depressor septi nasi. C: Compressor muscles: 6, transverse nasalis; 7, compressor narium minor. D: Minor dilator muscles: 8, dilator naris anterior. E: Other: 9, orbicularis oris; 10, corrugator.
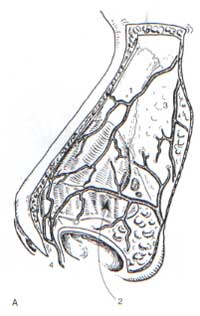
Figure 10. Nasal vasculature. 1, Dorsal nasal artery; 2, lateral nasal artery; 3, angular vessels; 4, columellar artery.
PEARLS
The nose may be thought of in anatomic thirds. The upper third roughly corresponds to the bony dorsum; the middle third roughly corresponds to the cartilaginous dorsum, and the lower third generally corresponds to the tip.
When describing relationships of one structure to another in the nose, use the well -defined anterior/posterior or caudal/cephalic. (Fig. 11).
The nasal bones are usually small; the ascending process of the maxilla provides a significant contribution to the bony anatomy of the nose.
The alar lobule contains fat and fibrous connective tissue, but it contains no cartilage. The lateral crus of the lower lateral cartilage takes on a more cephalic position as it extends laterally and is not found in the alar lobule.
The lobule, alar lobule, and the infratip lobule are terms that designate three distinct anatomic areas of the nose. The lower third of the nose may be referred to as the lobule or tip. The afar lobule is a fibrofatty nasal subunit that is devoid of cartilage and composes a portion of the lateral nasal sidewall. The infratip lobule
should comprise one third of the vertical length of the nose on base view (i.e., 2:1 columellar/lobule ratio).
The nasal valve area includes the cross-sectional area described by the nasal valve and is affected by the inferior turbinate, the caudal septum, and the tissues surrounding the pyriform aperture. The nasal valve proper is bounded by the nasal septum, the caudal margin of the upper lateral cartilage, and the floor of the nose, and is considered to be the location of the least cross-sectional area in the nose. In lateral osteotomies, care is taken to preserve a small triangle of bone at the pyriform aperture to prevent medialization of the inferior turbinate, which can compromise the cross-sectional area of the nasal valve area.
Scroll region: The upper lateral cartilages and lower lateral cartilages interrelate in three different configurations. Most commonly, the cephalic edge of the lower lateral cartilage overlaps the caudal edge of the upper lateral cartilage in the scroll region. Less commonly, the cephalic edge of the lower lateral cartilage abuts the caudal edge of the upper lateral cartilage. Rarely the cephalic edge of the lower lateral cartilage is overlapped by the caudal edge of the upper lateral cartilage.
Internasal suture line: The nasal bones are fused in the midline at the internasal suture. When elevating the skin-soft tissue envelope, decussating fibers must be divided (typically with scissors) from their attachment at the midline internasal suture to achieve the desired exposure.
The caudal margin of the nasal septum has a defined posterior septal angle, a middle septal angle, and an anterior septal angle. This anatomy plays a significant role in the shape of the nasal tip, including the infratip lobule, double-break, and supratip region. The surgeon attempting to create or allow for tip rotation by conservative excision of a superiorly based triangle of caudal septum must be aware of this anatomy.
The septum is composed of contributions from a number of anatomic structures (see Fig. 8).
In performing septoplasty, great care must be taken to preserve a generous L-strut to maintain support for the lower two thirds of the nose. Generally, it is recommended that at least 15 mm caudally and 15 mm dorsally (after accounting for any removal of dorsal hump) be preserved.
Rhinion versus sellion: The rhinion is the soft-tissue correlate of the osseocartilaginous junction of the nasal dorsum. The sellion corresponds to the osseocartilaginous junction of the nasal dorsum.
Osteotomies should not extend into the hard nasofrontal bone. When osteotomies extend too far cephalically into this thick, hard bone, a rocker deformity may result. In a rocker deformity, in-fracture of the bone may displace this excessive cephalic portion laterally.
Vascular supply and lymphatics are found superficial to the nasal musculature (2). The soft-tissue layers in the nose are epidermis, dermis, subcutaneous [this plane contains blood vessels and lymphatics, and also a (typically) thin layer of fat], muscle and fascia (musculoaponeurotic) plane, areolar tissue plane, and perichondrium/periosteum. Dissection during rhinoplasty in the proper tissue planes [areolar tissue plane (i.e., submusculoaponeurotic)] preserves nasal blood supply and minimizes postoperative edema.
The astute surgeon will be able to anticipate the contour of the upper and lower lateral cartilages by studying the surface topography of the nose.
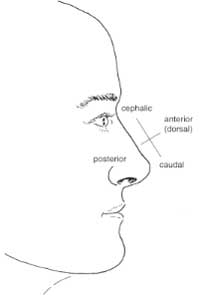
Figure 11. Nasal relationships.
REFERENCES
Tardy ME. Brown R. Surgical anatomy of the nose. New York: Raven Press, 1990.
Toriumi DM. Mueller RA, Grosch T, BhattacharvyaTK, Larrabee WF. Vascular anatomy of the nose and the external rhinoplasty approach. Arch Oto/ Head Neck Surgery 1996:122:24-34.