Proper local anesthesia is critical to allow atraumatic dissection with minimal bleeding and edema. A total volume of less than 3 ml of 1% lidocaine with 1:100,000 epinephrine is typically used to attain anesthesia for rhinoplasty alone. When performing septorhinoplasty, as much as 10 nil of local anesthetic may be used. The anesthetic is al- lowed to take effect for at least 15 minutes to maximize the vasoconstrictive effect of the epinephrine.
To become familiar with a method of injection of local anesthetic agent, saline can be injected with a 5-ml syringe and 27 gauge (1.5 cm) needle along the site of injection in a cadaver specimen. Injection varies in some respects, based on the surgical approach selected; for example, the subdermal columellar injection may be omitted in an endonasal approach. A generalized approach to injection is described below. For a septoplasty, multiple 0.5-m1 to 1.0 ml injections are made in the subperichondrial and subperiosteal plane along the entire area of anticipated dissection. Injections also should be placed along the site of the proposed incision (Killian, hemitransfixion, etc.). Both sides of the septum should be injected if the surgeon plans to elevate mucosa bilaterally. The injection will aid in the dissection if placed in the subperichondrial plane. It is helpful to place an injection on the posterosuperior septum bilaterally to minimize bleeding from the sphenopalatine blood vessels.
Inject local anesthetic into the subdermal plane in the midline of the columella from tip – defining points to the nasal spine in preparation for the external approach (Fig. 1 ). This injection is limited to <0.3 ml to prevent distortion of the columella or nasal base.

Figure 1. Inject <0.3 ml of local anesthetic into the subdermal plane in the midline of the columella from tip-defining points to the nasal spine in preparation for the external approach. This injection of the columella is necessary for the external approach but may not be necessary for most endonasal approaches.
For either endonasal or external approach, inject <0.3 ml of local anesthesia into the soft-tissue between and around the domes of the lower lateral cartilages (Fig. 2). The injection extends up to the region of the anterior septal angle. After completing this injection, gently massage the domal region between the thumb and index finger of both hands to disperse the anesthetic throughout the tip region.
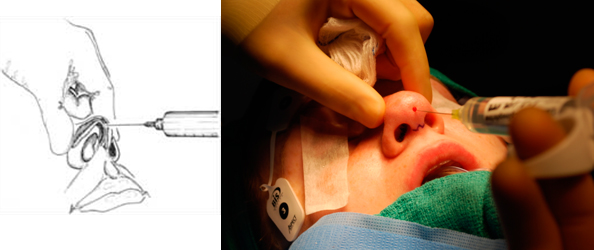
Figure 2. Inject <0.3 ml of local anesthetic into the soft tissue between the domes of the lower lateral cartilages. Injection of the supratip is illustrated here as a percutaneous injection but also may be performed endonasally.
Place multiple injections of 0.1 ml of local anesthetic along the caudal margin of the lateral and intermediate crura (along the planned marginal incision; Fig. 3). Overinjection will result in distortion of the nostril rim and soft-tissue triangle.


Figure 3. Place multiple injections of 0.1 ml of local anesthetic along the caudal margin of the lateral and intermediate crura (along the planned marginal incision).
Inject <0.1 ml to raise a small bleb in the vestibular skin along the lateral aspect of the medial crura, at the planned incision site for the columellar flap of the external rhinoplasty approach (Fig. 4).
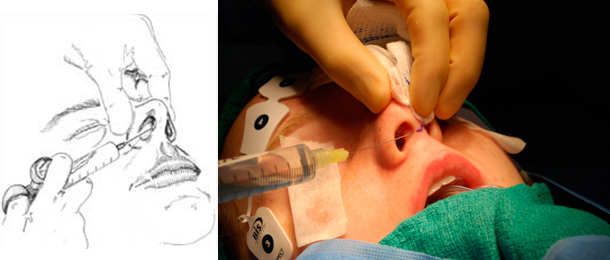
Figure 4. Inject <0.3 ml along the planned incision site for the columellar flap of the external rhinoplasty approach.
For an intercartilaginous, transcartilaginous, or delivery approach, place similar injections of 0.1 ml intranasally along the respective incision sites (Fig. 5).

Figure 5. For an intercartilaginous, transcartilaginous, or delivery approach, place injections of 0.1 ml intranasally along the incision site.
After inserting the needle between the upper and lower lateral cartilages (intercartilaginous), inject local anesthetic along the lateral wall of the nose approximately 1 cm off the 4 midline (Fig. 6). The line of injection is along the lateral aspect of the nose and extends from the nasofrontal suture line to the cephalic margin of the lateral crura. Use <0.5 ml for this injection to prevent distortion of the tissues. Perform no injections along the dorsum of the nose to prevent distortion of the soft tissue that may inhibit accurate evaluation of the contour of the dorsum. In preparation for lateral osteotomies, inject on the outside and in-side of the nasal bones just above the periosteum. After completing these injections, massage the injection sites to help disperse the local anesthetic and prevent tissue distortion.
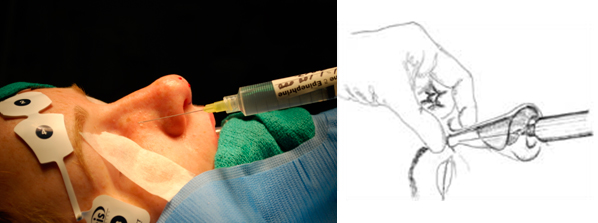

Figure 6. A. Injection of local anesthetic along the lateral wall of the nose. B. Injection for lateral osteotomies.
PEARLS
- Subperichondrial and subperiosteal injections of local anesthetic will make dissection of the septal flap easier by hydrodissecting the flap. This is particularlyhelpful when dissecting over fractures in the cartilage, bone, or along the maxillary crest.
- Injection of the osteotomy sites should be performed on the inside and outside of the ascending process of the maxilla.
- Avoid excessive injection of local anesthetic into the columella: otherwise the relation between the ala and columella may be altered.
- In cases in which dorsal hump excision must extend into the region of the nasofrontal angle, additional injections of local anesthetic can be placed along the path of the supratrochlear artery and just medial to the medial canthus.
- If the surgeon plans to use lateral crural strut grafts, injections of local anesthetic can be placed in the vestibular skin on the undersurface of the lateral crura where the vestibular skin will be dissected.
REFERENCES
- Beeson WH. The nasal septum. Otolarvngol Clin North Amer 1997;20:743-767.
- Kasperbauer JL, Facer GW, Kem EB. Reconstructive surgery of the nasal septum. In: Papal ID, Nachlas NE, eds. Facial plastic and reconstructive surgery. Philadelphia: Mosby Year Book, 1992:337-343.