The internal approach in rhinoplasty requires a surgical experience and an artistic perspective to provide adequate results on nasal deformities. The external approach allows cartilage shaping and grafting through a wider exposition of the entire nasal structure (bones and cartilages), but leaves a columellar scar. The wide marginal approach is known as open rhinoplasty without skin-columella incision. It was first described by guerrerosantos [1] in 1987. This procedure was originally introduced to lessen the complications seen with the open approach, while keeping the advantages of a better exposition insufficient with closed rhinoplasties. Although scarcely discussed in the literature, this approach can be proposed to a patient refusing the open approach when needed to address difficult tips.
Surgical technique:
The nasal tip is infiltrated with 2% lidocaïne and epinephrine. The incision is longer than the one described by guerrerosantos [1]. It includes the incision described by holmstrom [2] (fig.1). The incision is carried out on both sides; it starts 2 mm under the medial crus (fig.2) and continues along the alar cartilage margin following the borders of the lateral crus to the domal region, it ends at the nostril. The incision should not be circular and must leave 15 mm of unarmed mucosa in the area of the nasal floor. The dissection is done with scissors carefully avoiding injury to the medial crus and creating a columellar communication (fig. 4). Submucosal dissection enables good vision of the upper lateral cartilage, the alar domes can thus be exposed, and the interdomal ligament is severed giving access to the cartilaginous septum that can be freed up to bone-cartilage junction. The wide marginal approach is now completed and the work on the alar cartilages and the grafting can take place (fig. 6,7,8,9,10) according to the needs of each case. The incision is then sutured with 5/0 fast absorbing gut.
Discussion :
Tip surgery is usually a challenge in rhinoplasty. The surgeon has the choice between open or internal approach [3]. The internal approach has unique internal incisions that do not scar the columella and has a good aesthetic evaluation. The open approach gives a better access to the bony and cartilaginous structure of the nose, but leaves a scar on the columella. This approach separates the nasal skin from the bones and cartilage, and limits the evaluation the dorsum and the projected tip. The section of the lymphatic and venous drainage provokes a lasting oedema of the tip. The internal approach is uncomfortable for the surgeon and the open approach is uncomfortable for the patient. For these reasons, a surgical alternative is proposed. It should enable a wider exposition of the cartilaginous tip without the columellar incision. Guerrerosantos [1] and holmstrom [2] were the first to describe this wide marginal incision technique and publish their results. This technique remains an internal approach as opposed to the open external approach. The wide marginal approach is probably used implicitly by surgeons who extend their internal incisions during the procedure. This approach allows work on the cartilage junctures of the nose and on the dorsal hump if needed (rasp or osteotomies). Lateral osteotomies are done in an ascending motion with curved ostetomes. Tip correction and common procedures on the nasal tip is easy through the wide marginal approach [4]. Tip grafting with several types of grafts is possible, including spreader graft, strut graft, and shield graft. The wide marginal approach is to be considered when difficult nose tip work is planned during surgery. It is an acceptable alternative when facing patients refusing a columellar incision, or in case of difficulties during an internal approach procedure.
Literature
1. GUERREROSANTOS J. Open rhinoplasty without skin-columella incision. PLAST RECONSTR SURG. 1990 Jun;85(6):955-60.
2. HOLMSTRÖM H, LUZI F. Open rhinoplasty without transcolumellar incision. PLAST RECONSTR SURG. 1996 Feb;97(2):321-6.
3. SHEEN JH. Closed versus open rhinoplasty : and the debate goes on. PLAST RECONTR SURG. 1997;99(3):859-862.
4. TARDY ME , PATT BS, WALTER MA. Transdomal suture refinement of the nasal tip: long-term outcomes. FACIAL PLAST SURG. 1993 Oct;9(4):275-84.
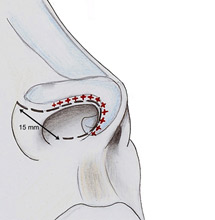 | Figure 1: +++++ marginal incision, ——- wide marginal incision, incision leaves about 15 mm intact in the lateral area of the nasal floor |
 | Figure 2: Incision starts in the foot of the medial crus inside the margin of the columella |
 | Figure 3: Incision goes on marginal rim of the alar cartilage and follows the border of the lateral crus |
 | Figure 4: Complete transfixion incision |
 | Figure 5: Detachment of the mucous from the the medial and lateral crus is performed until the triangular cartilage is shown |
 | Figure 6: Both alar domes are exposed |
 | Figure 7: Each side of the marginal approach allows an exposition of the cartilage pyramid |
 | Figure 8: Resection of the cephalic parts of the lateral crus |
 | Figure 9: Placing of the sutures between medial and lateral crus, thereby reconstructing interdomal ligament |
 | Figure 10: Positioning a shield-type tip graft |
 |  |
| a | b |
 |  |
| c | d |
 |  |
| e | f |
 |  |
| g | h |
Figure 11a-h: Pre- and post-operative views of a patient with a bulbous tip with lack of projection, who underwent a resection of the cephalic parts of the lateral crus with transdomal suture and a hump resection.