INTRODUCTION
The overprotected nose, also known as the “Pinocchio nose”, is a frequent reason for consultation in the daily practice of a facial plastic surgeon. In this group of patients, the nose becomes the main point of the attention of the face due to its larger dimension and often results in the loss of balance of the other facial structures (1) (2). This brings the stigmatization of an individual and in some cases to impairment of self-esteem and poor social interaction.
When this situation is generated by the size of the alar cartilages, it is necessary to reduce them in surgery to decrease the nasal tip projection.
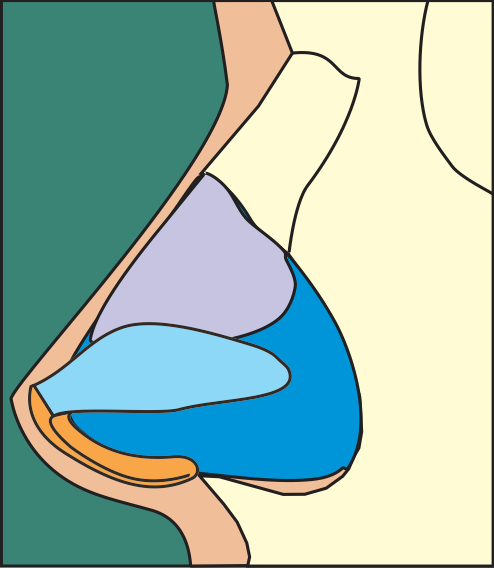
It is essential to remember the concept of the nasal tip tripod (3) (4), in which the medial crus correspond to the central support, the lateral crus are the lateral support and the apex where both crus join is the nasal dome. (Figure 1)
There are numerous techniques described to deproject the nose, most of them involve a high technical difficulty or require an important modification of the morphology of the alar cartilages that may generate long-term irregularities and instability.
This article describes a new deprojection technique, easily reproducible, that does not modify the tip rotation and preserves cartilaginous stability.
CHARACTERISTICS OF THE NASAL TIP
An aesthetically pleasing nose should be symmetrical, with smooth and balanced contours in its upper, middle and lower thirds, should be consistent with the other features of the face and always has to be evaluated as a whole. (5)
Many characteristics of the nose must be evaluated when performing an aesthetic analysis. These are indispensable in the surgical planning of rhinoplasty:
- Projection: Refers to the location of the nasal tip on the horizontal axis.
- Rotation: Corresponds to the location of the nasal tip on the vertical axis.
- Definition: Thickness of the skin that allows perceiving the architecture of the cartilages that give shape and form to the nasal tip and the transition zones between the tip and the alar lobe.
- Nasal length: Distance between nasion and the tip of the nose.
- Nasal width: Width of the tip and the nasal dorsum in the anteroposterior view of the face.
DIAGNOSIS OF THE OVERPROJECTED NOSE
To make an accurate diagnosis of an overprotected nose, the degree of projection of the nasal tip should be determined. Several ways of measurement and normality ranges have been described in the literature as the measurement of the distance from the point where the nose joins the face at the level of the nasion, the rinion and the nasal tip, whose corresponding values are: 9-14 mm, 18-22 mm and 28-32 mm respectively.
There are other ways to determine the projection of the nose. Among the most used are those described by:
- Goode: Establishes that the projection of the tip should be between 55 – 60% of the length of the nose. A vertical line is drawn between the nasion and the facial alar groove, and from there a perpendicular line is drawn in the direction of the nasal tip. (6)
- Simons: The distance between the subnasal point to the nasal tip equals the length of the upper lip. (7) (8)
- Byrd: It states that the projection should be equal to 2/3 of the patient’s ideal nasal length. (9)
Another point of great importance is to define the anatomical structure responsible for nasal overprotection, with hyperdeveloped alar cartilages being the more common reason; however, there are other situations that can give the appearance or simulate an overprotected nasal tip (10), when the actual projection is normal.
Among the non-nasal causes that can give the appearance of an over projected tip are the small chin and the presence of an upper maxillary bone overdeveloped. (11) Among the nasal causes that can give the appearance of a overprojected tip are the following: a short radix, a prominent nasal dorsum, an overdeveloped caudal septum and a prominent anterior nasal spine (12) (13) (figure 1)

There are several mechanisms that held the nasal tip in position, these mechanisms were initially described by Janeke. (14) (figure 2)
SUPPORT MECHANISMS OF THE NASAL TIP
Major Support Mechanisms:
- Strength and elasticity of the alar cartilages.
- Union of the alar cartilages to the upper lateral cartilages.
- Binding of the alar cartilage to the cartilaginous septum.
Minor Support Mechanisms:
- Anterior nasal spine.
- Membranous septum.
- Interdomal ligament.
- Union of the alar cartilage to the skin.
- Dorsal cartilaginous septum.
- Sesamoid complex.
This article aims at the treatment of over projection of the nasal tip through the modification of the size of the alar cartilages (Figure 3).

DEPROJECTION TECHNIQUES OF THE NASAL POINT
Nasal tip deprojection techniques can be classified according to the intervened structure in: (figure 4)
- Weakening of the Nasal Tip Support Mechanisms
Preseptal transfixing incision, anterior septal angle management, alar cephalic trimming, anterior nasal spine resection.
- Intervention in the projection of the medial crus (15) (16)
- Septocolumelar suture.
- Suturing of medial crus to septum (Tongue in Groove).
- Decrease in the length of the medial crus by resection of the crus footplates.
- Lipsett technique (17) deprojection of the tip by excision of a portion of medial crus with the vestibular skin that covers it and the creation of new domes.
- Cut and overlay of the medial crus.
- Cutting of the domes and formation of new ones, Dome truncation (Goldman technique). (18)
- Intervention in the projection of the lateral crus. (19)
Cut and overlay of lateral crus.
- Intervention in middle and lateral crus.
- Cut of meddle and lateral crus.
- Alar setback (20): symmetrical excision of a medial crus portion, without compromising the vestibule skin and the remaining crus ends sutured to an intercrural strut. Then the lateral crus are divided and overlapped, fixing them according to the desired rotation.
- Sliding technique (21) (22): sliding of the medial or lateral crus, generating caudal or cranial rotation, respectively.
Although there are various techniques for over projected nose management, most of them have some limitations that must be taken into consideration.
The techniques related to the modification of the nasal tip support mechanisms are useful in those cases in which a minimum projection is needed; however, their results are not easily predictable.
The cutting of the domes or their truncation, if not properly repaired, can produce irregularities and asymmetries of the nasal tip (23).
The techniques that only treat one of the crus (medial or lateral) without modification of the position of the domes produce an alteration of the nasal tip rotation. (24)
Those techniques in which both crus are cut and repaired are effective in reducing the size and projection of the nasal tip; however, they are technically complex and can generate instability of the alar cartilages with a tendency to collapse of the internal nasal valve. This happens mainly in those cases in which an end-to-end suture is performed, since the space between cartilages will only have fibrous tissue that has less resistance to collapse by the negative pressure of nasal breathing.
Gubisch and Eichhorn-Sens described the sliding technique to achieve a deprojection of the nasal tip. In their description they mention the different variants of the sliding principle (medial, lateral and combined), which consists in establishing different points with specific measures in the medial or lateral crus, which define the cartilage cutting area and the level of overlapping. Within the benefits of the technique, are the possibility of correcting the cartilage malformations and strengthening the anterior pillar by the cartilage superposition in the medial variant or with the use of a strut graft in the lateral variant (22) (21).
Neu proposes the realization of “medial rotation of the alar cartilage”, which consists on moving the dome towards the lateral crus (lateralize) between 5-6 mm; then, slide the elongated medial crus towards the anterior nasal spine over the caudal septum. The excess of cartilage in the medial crus is resected (5-6mm) at the level of the footplate. This technique combines the mobilization of the dome with a cut of cartilage. The advantage of this technique is that the structural integrity of the alar cartilages is preserved. (25)
In general terms, there are overlapping techniques and excisional techniques (cartilage trimming). We consider that the former is more suitable in rhinoplasty since this allow preserving cartilage and the support of the nasal pyramid.
FUNDAMENTAL CONCEPTS OF THE TECHNIQUE
1. To deproject the nasal tip without changes in rotation, the three pillars of the Anderson tripod must be symmetrically intervened, that is, the medial pillar composed of both medial crus and the two lateral crus of the alar cartilages.
2. For every millimeter diminished in length of each crus, the nasal tip is deprojected one millimeter.
3. The movement of the dome towards the medial crus (medialization) generates a shortening of the medial crus and the extension of the lateral crus. For every millimeter of medial displacement of the dome, the length of the lateral crus are increased by one millimeter
4. If we want to deproject the dome, we can cut the medial crus and the lateral crus in an equal quantity of millimeters or we can medialize the dome and cut only the lateral crus the double of millimeters without cutting the medial crus.
5. The cut and overlap of the lateral crus with suture achieve a shortening of the crus and increases its rigidity thanks to this superposition.
The following formula follows:
Deprojection required (X mm) = medial crura reduction (X mm) and lateral crura reduction (X mm)
This procedure gives the same result as:
Deprojection required (X mm) = Dome medialization (X mm) + trimming and lateral crura overlap (2 * X mm)
SURGICAL TECHNIQUE: DEPROJECTION
This technique can be performed using an open or closed approach.
Adequate surgical planning should be performed in the office next to the patient to establish the desired degree of nasal tip projection.
The alar cartilages domes are identified and marked with methylene blue.
The dome is going to move from lateral to medial (medial crura steal) the number of millimeters that we want to reduce the projection. There we made a new mark.
Once the position of the new dome is defined, the place where the lateral crus section is marked. This section must be at least 10 mm from the new dome.
The vestibular mucosa of the lateral crus is dissected and the lateral crus is cut transversely.
After cutting the lateral crus, the two segments are overlapped twice as many millimeters as it is desired to reduce the projection of the dome and they are secured with 6 zero polypropylene suture.
Once the length is reduced in the alar cartilage, transdomal suture are placed to fix the position of the new dome and the same maneuver is performed on the contralateral cartilage. (Figure 5 and 6)
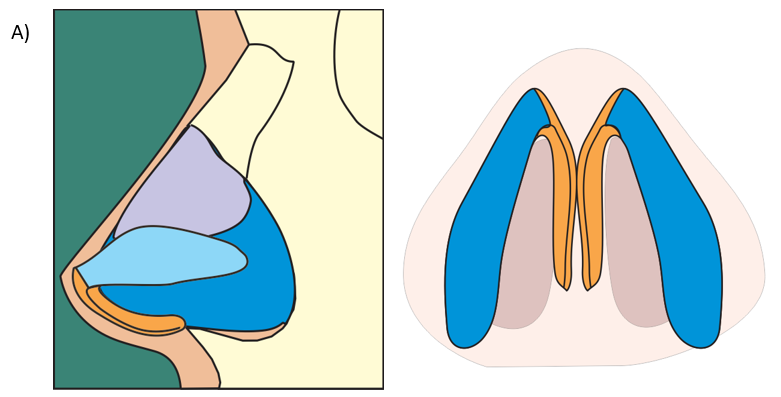
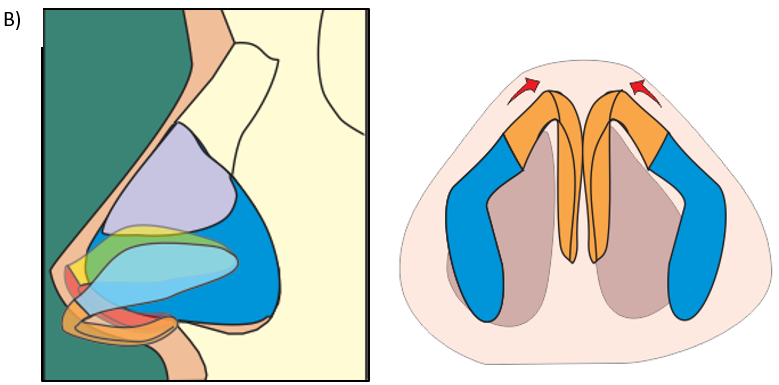
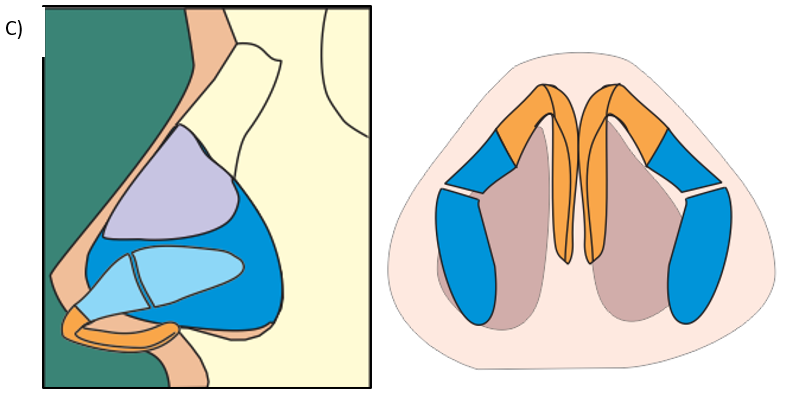
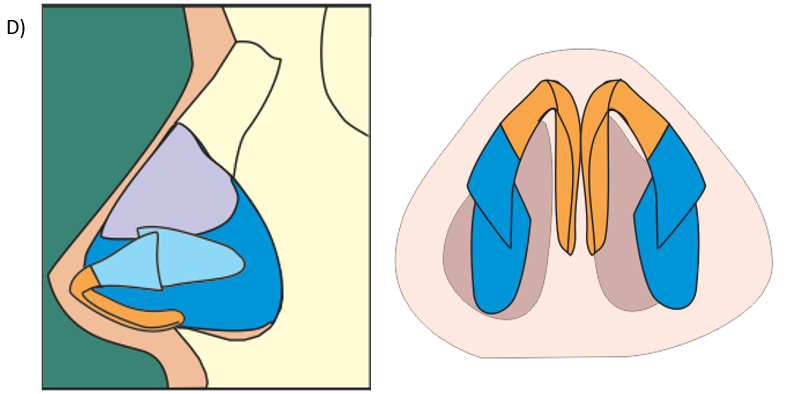
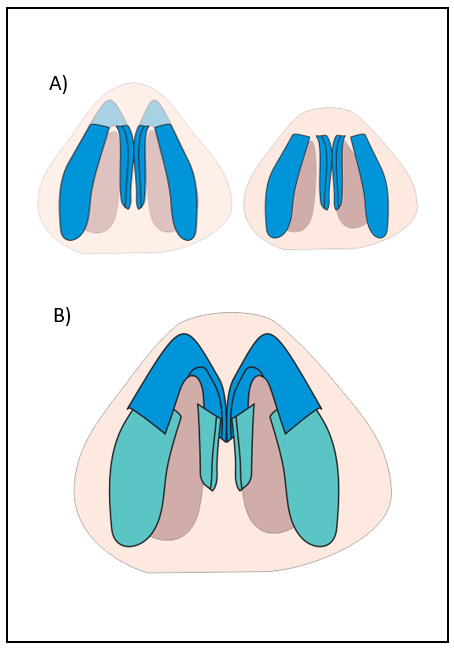
Figure 5. A) Visualization of the alar cartilages with its base configuration. B) Represents what would happen if only a medialization of the dome (medial crura steal) were carried out. There is an inferior rotation of the nasal tip and a lengthening of the lateral crura. C) Cross-section of the lateral crura 10 mm from the new dome. D) Overlay of lateral crura obtaining the reduction of the projection of the dome.
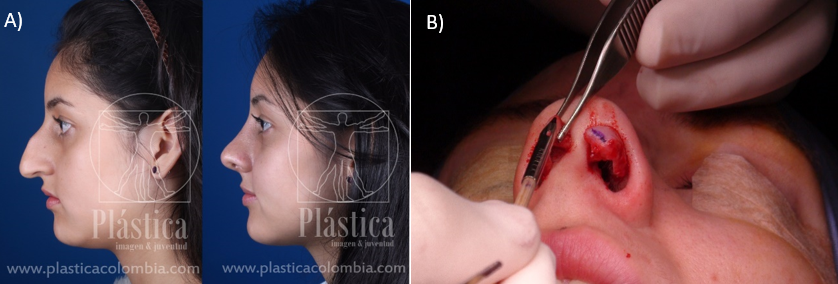
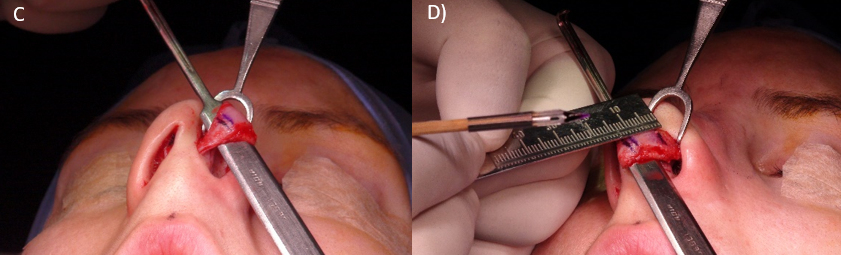
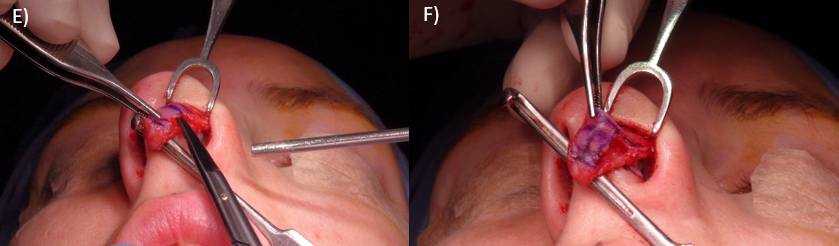
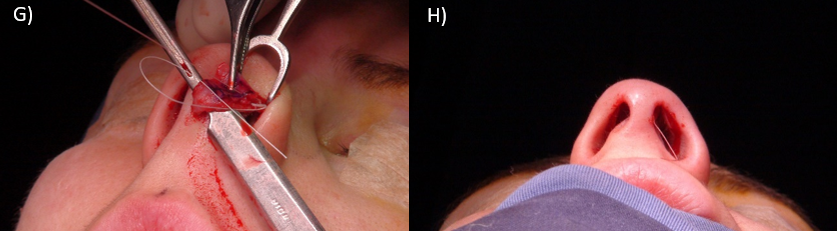

Figure 6. A) Photograph of before and after performing a rhinoplasty in a patient with an over projected nose. B) Dome marking with methylene blue. C) Medial marking of a new dome (medial crura steal). D) Marking of lateral crus 10 mm from the new dome. E) Dissection of the vestibular mucosa under the lateral crus. F) Incision of the lateral crus. G) Overlay of lateral crus. H) Deprojected left dome, that the difference in projection of the domes is immediately noticed. The right dome with normal projection and the left one already diminished in projection. I) Both domes deprojected (the tip is remains wide because the transdomal and interdomal sutures have not been placed yet).
DISCUSSION
The over projected nose represents an important challenge for the surgeon. Adequate knowledge of the nasal anatomy is required to make an accurate diagnosis of the involved structures.
For the realization of this article, we focused on hyperdeveloped alar cartilages and their clinical manifestation: overprojected nasal tip. For the correction of this entity, exist multiple surgical techniques that aim to achieve a retro-displacement of the Anderson´s tripod mentioned previously; however, many of these techniques bring problems for the patient (irregularities of the nasal tip, nasal valve collapse) or for the surgeon (difficulties in performing the surgical technique) (3).
By using the dome medialization technique combined with the lateral crus overlay, we can be achieve a precise deprojection of the nasal tip as planned in the office consultation. In addition, we consider it a simple, fast and reproducible technique.
Some of the advantages that this technique has: 1) it provides structural stability of the alar cartilage. 2) It requires the manipulation of one crus (lateral crus). 3) Reduced surgical time. 4) The overlap of lateral crus allows treating the excess length of this segment and its curvature, avoiding the widening of the nostrils and the requirement of other procedures.
CONCLUSION
There are many surgical techniques designed for the management of the overprotected nasal tip. The use of deprojection techniques has to be individualized according to the needs of the surgeon and taking into account the anatomy of the patient (alar cartilage morphology, skin type, etc.).
We consider that the medialization of the dome together with the overlapping of the lateral crura is a simple and easy measure to correct this entity.
Bibliography
- The overprojecting nose: anatomic component analysis and repair. . Tardy, ME, Walter, MA and Patt, BS. 1993 9 (4), Facial Plast Surg, p. 306-316.
- Population-Based Assessment of Currently Proposed Ideals of Nasal Tip Projection and Rotation in Young Women. Ahmed, O, and others. 5, 2014, JAMA Facial Plast Surg, Vol. 16, p. 310-318.
- Anderson, JR. The dynamics of rhinoplasty. Preceedings of the Ninth International Congress of Otorhinolaryngology. Mexico city: Bustamant GA, August 10-14, 1969.
- Tripod resection for ‘‘ Pinocchio ’’ nose deformity. Fredericks, S. 1974, Plast Reconstr Surg, Vol. 53, p. 531-533.
- New concepts in nasal tip contouring. Toriumi, D and Checcone, M. 1, 2009, Facial Plastic Surgery Clinics of North America, Vol. 17, p. 55-90.
- Goode, RL. A method of tip projection measurement. [aut. book] N Powell and Humphreys B. Porportions of the aesthetic face. New York: Thieme-Stratton, 1984, p. 15-39.
- Nasal tip projection, ptosis and supratip thickening. Simons, RL. 1982, Ear Nose Thorat J, Vol. 61, p. 452-455.
- Vertical dome division in rhinoplasty. Simons, RL. 4, 1987, Otolaryngol Clin North Am, Vol. 20, p. 785–796.
- Rhinoplasty: a practical guide for surgical planning. Byrd, Hs and Hobar, PC. 4, 1993, Plast Reconstr Surg, Vol. 91, p. 642-654.
- Universal Retraction Suture for the Overprojecting Nasal Tip. N, Fanous, and others. 3, 2010, Canadian Journal of Plastic Surgery, Vol. 18, p. 99-106.
- A Multivariate Analysis of Nasal Tip Deprojection. Unger, J, and others. 2012, Plastic and reconstructive surgery, Vol. 129, p. 1163-7.
- Projection and Deprojection Techniques in Rhinoplasty. Fazil, Apaydin. 1, 2016, Clinics in Plastic Surgery, Vol. 43, p. 151-168.
- Deprojection of the Nasal Tip in Revision Rhinoplasty. Kridel, R y Undavia, S. 04, 2012, Facial Plastic Surgery, Vol. 28, p. 440-446.
- Studies on the Support of the Nasal Tip. Janeke, JB and Wright, WK. 5, 1971, Archives of Otolaryngology – Head and Neck Surgery, Vol. 93, p. 458-464.
- Nasal tip sutures: Techniques and indications. Cingi, C, and others. 6, 2015, American Journal of Rhinology & Allergy, Vol. 29, p. 205-211.
- Comparison of Tongue-in-Groove and Columellar Strut on Rotation and Projection in Droopy Nasal Tip: Contribution of a Cap Graft. Demir, UL. 00, 2017, J Craniofac Surg, Vol. 00, p. 00-00.
- A New Approach to Surgery of the Lower Cartilaginous Vault. Lipsett, EM. 1, 1959, Archives of Otolaryngology – Head and Neck Surgery, Vol. 70, p. 42–47.
- Surgical tips on the nasal tip. Goldman, IB. 1954, Ear Nose Throat J, Vol. 53, p. 583.
- Nasal Tip Deprojection with Crural Cartilage Overlap: The M-Arch Model. Sands, NB and Adamson, PA. 1, 2015, Facial Plast Surg Clin N Am, Vol. 23, p. 93–104.
- Alar Setback Technique: A Controlled Method of Nasal Tip Deprojection. Foda, HMT. 11, 2001, Arch Otolaryngol Head Neck Surg., Vol. 127, p. 1341–1346.
- The Sliding Technique: A Method to Treat the Overprojected Nasal Tip. Gubisch W, Eichhorn-Sens J. 5, 2008, Aesth etic Plastic Surgery, Vol. 32, págs. 772–778.
- The sliding technique. A precise method for treating the overprojected nasal tip. Eichhorn-Sens, J y Gubisch, W. 12, 2009, HNO, Vol. 57, págs. 1262-72.
- A New Twist in Nasal Tip Surgery: An Alternative to the Goldman Tip for the Wide or Bulbous Lobule. McCollough, EG y English, JL. 8, 1985, Arch Otolaryngol, Vol. 111, págs. 524–529.
- Anatomical Study of the Medial Crura and the Effect on Nasal Tip Projection in Open Rhinoplasty. Patel, K, y otros. 2014, Plast. Reconstr. Surg., Vol. 132, págs. 787-793.
- Reduction of nasal tip projection with medial rotation of alar cartilages. Neu, BR. 3, 2001, Plast Reconstr Surg, Vol. 108, págs. 763–767.