Keywords: Rhinoplasty, nasal tip, projection, tongue in groove.
Background
The aesthetic surgical mastery of the lower third of the nose has long been recognised as one of the most challenging parts of doing rhinoplasty. Rhinoplasty surgeons use a variety of surgical techniques to obtain the desired aesthetic results. Surgeons over the years have tried a variety of novel techniques to help refine, rotate and project the nose. Despite advances in the knowledge of nasal anatomy and the ongoing development of new techniques, nasal tip modification remains a challenge. Many of the rhinoplasty manoeuvres which are traditionally used can result in loss of tip support.
The tongue-in-groove (TIG) technique is normally used in combination with other techniques. It is a conservative but powerful surgical suture technique that allows control of nasal tip rotation and projection, can correct columellar show and can straighten a caudal septal deviation.[1][2][3]
Historical development of tip modification techniques
Surgery of the nasal tip remains one of the most challenging aspects of aesthetic nasal surgery. The main characteristics of the nasal tip can be described in terms of shape, rotation and projection. Mechanisms of supporting the nasal tip have been well described (see Table 1).[4] Traditional rhinoplasty approaches violate most, if not all of them.
Even in the time of Jacques Joseph in the 1930s, it was known that most rhinoplasties resulted in the loss of tip projection. He compensated for the loss of tip projection by lowering the dorsum. For decades excessive removal of the nasal dorsum to compensate for the loss of tip projection resulted in undesirably small noses. Subsequently, techniques were developed to maintain and if necessary increase tip projection. This can be done by enhancing the height of middle crura by vertical dome division type techniques. [5][6][7]Cartilage tip grafts applied either as shields or as onlay grafts are strong instruments to increase nasal tip projection.[8][9] Alternatively, one may increase the length of medial crura by using a strut inserted in between the medial crura reaching up to but not resting on the nasal spine.[10][11] Columellar struts give support to the medial crura but do not increase the nasal tip projection and hence they are often combined with tip grafts.[8][12] If maximum support is needed for tip projection, a strut may be fixed on the nasal spine.[13]
Different suture techniques attaching the medial crura to the septum directly or to a caudal septal extension graft have been described.[14][15] Alternatively, Kridel and Foda suggested increasing the height of the medial crura by borrowing from the lateral crura the so-called lateral crural steal technique.[16][17] This may be considered as an alternative to the vertical dome division technique.
History of Tongue-in-Groove
The name tongue-in-groove gained popularity in 1999 when Kridel described the technique along with a 10-year clinical experience, in which 97% of his long-term follow-up patients were happy functionally and aesthetically.[1] The TIG technique, in essence, is a repositioning technique of both medial crura around the caudal septum. Although the name is unconventional as a surgical name, it fits the principal perfectly. The groove is a surgically created space between the medial crura and membranous septum, and the tongue is the caudal border of the nasal septum. The technique can be carried out through a closed or open approach. Since 1999, several articles have been published referring to TIG as a technique to adjust the alar-columellar relationship (columellar show), to help modify a droopy tip, to support septal extension/columellar strut grafts, or enhance tip support, projection and rotation.[1][2][3][18][19] TIG delivers a high degree of patient satisfaction with predictable results and few complications (see Table 2).[2]
Surgical Details [2]
Preparation for Tongue-in-Groove in External Rhinoplasty
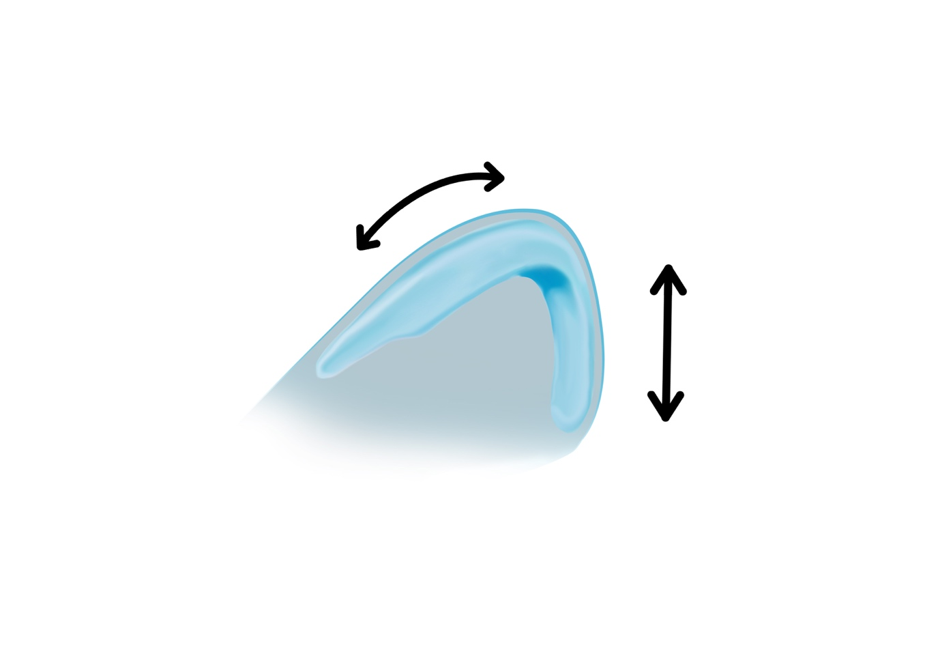
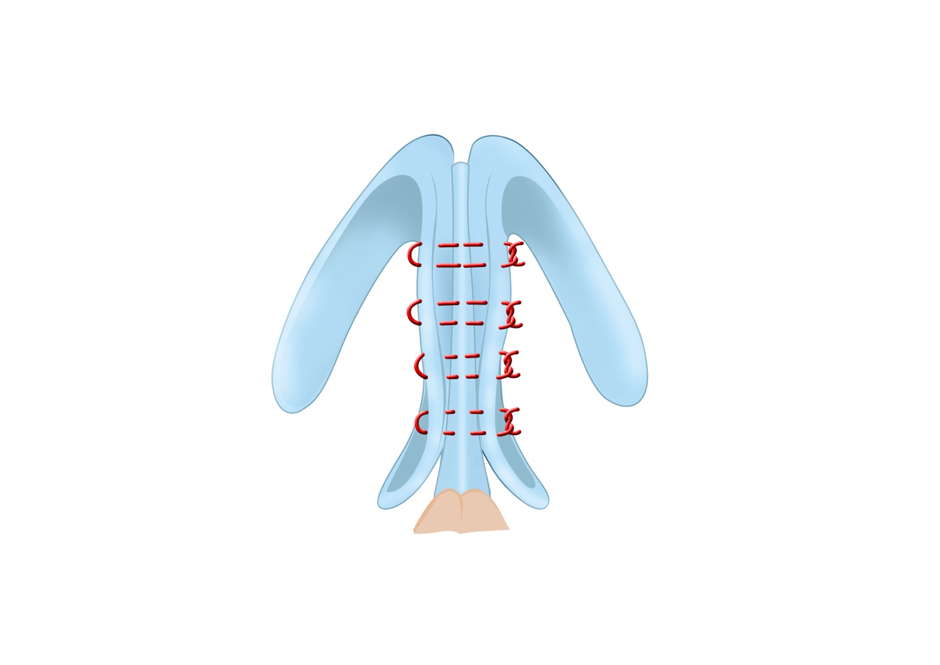
Although the procedure can be done through an endonasal approach, the open technique provides most accuracy, speed and ease. Patients should have prior standard pre-operative rhinoplasty photographs taken. A mid-columellar inverted V-shaped incision is made. This incision is extended bilaterally into marginal incisions along the caudal edge of the lateral crura. The skin and soft tissue envelope are raised, and the cartilage framework is exposed. The medial crura and caudal end of the septum are exposed. The two medial crura are moved forwards or backwards onto the caudal septum so as to achieve the desired nasal tip position (Figure 1), and the structures are fixated into position with sutures. The medial crura are fixed directly to the caudal septum (Figure 2), or alternatively if the septal cartilage is not long enough they are sutured to the cartilage of a septal extension graft fixed to the caudal end of the septum (Figure 3). Septal extension grafts are required in short noses or cases with deficient septal length where the caudal extension of the septum is not sufficient for the TIG technique.

Tongue-in-Groove Suturing
Once a stable tongue is created to support the nasal base, the next step is to adjust the medial crural position, to achieve the desired rotation, projection, and columellar show, and the medial crura are securely sutured to the caudal septum. It is the author’s preference to use 4/0 PDS for this. The soft tissue/skin envelope is re-draped to give visual feedback of the new shape and position of the nasal tip.
Additional Tip Techniques
In most cases, TIG is sufficient to control the tip orientation. But sometimes additional rhinoplasty techniques are needed on top to help with tip adjustment, these can be used in combination with TIG. To help deproject the nose we can utilise medial crural setback, footplate resection and medial crural overlay. Following the medial crura being sutured and fixed in TIG, this can incidentally lead to lateral crural flaring. Often a release incision of the lateral crura in the hinge area and relocation into a pocket can release tension and prevent flaring of the lateral crura and resolve this issue. When a release incision is insufficient then a lateral crural overlay procedure can be performed. In some cases, a shield graft can be used to further increase tip projection, or adjust the infratip contour.
Often, patients will have a cephalic trim, scroll excision and domal suturing at the same time as the TIG, which can contribute to tip rotation.[20]
Advantages and Disadvantages of Tongue-in- Groove
The main advantage of TIG technique is that it creates predictable long-term aesthetically and functionally good results. Patient postoperative satisfaction studies appear to reaffirm this.[19]
Other advantages are the surgeon gets immediate on the table visual feedback on tip projection and rotation. in other words “what you see, is what you get”. Secondly, as the lobular cartilaginous framework remains intact, this allows reversibility and fine-tuning of the medial crural position. Thirdly, as there is a bringing together of three layers of cartilage, this increases nasal base support and thus minimises the risk of support failure. Lastly, TIG is a relatively simple technique to master, is suitable in open and closed cases, suitable in revision cases, and can easily be combined with other rhinoplasty manoeuvres.
The main disadvantage of TIG is a rigid nasal tip with the static appearance of the nose during facial expressions. Tip stiffness should be mentioned to the patient pre-operatively. Columellar cellulitis and suture granuloma have been reported. TIG relies on a stable tongue, so a well supported septal L-strut, septal extension, or columellar strut is essential.
Tongue-in-Groove in Revision Rhinoplasty
Revision rhinoplasty is a difficult endeavour. The success depends on stability and presence of the cartilaginous framework. For dorsal support and internal valve restoration, spreader grafts may be used. Extra-long spreader grafts allow fixation of a septal extension graft which can be easily combined with TIG to stop graft deflection and improve stability to the nasal base. TIG allows predictable and reliable restoration of tip projection and rotation.
Discussion
Two decades after tongue-in-groove was popularised by Kridel, today the term is embedded in modern rhinoplasty literature. Its unconventional name fitting what it does perfectly. The surgical space between the conjoined medial crura forming the “groove”; which can be sutured onto the “tongue”, being either the caudal septum or a septal extension graft. TIG is used to stabilise the nasal base, to set tip projection and rotation, and correct the alar-columellar relationship. It is a forgiving, predictable and reversible technique which ticks all the boxes for modern concepts of rhinoplasty; it is better to conserve and relocate, rather than to resect and regret. Literature shows that long term success rates of TIG are high and complications are low.[19]
There is no preference for an open or closed approach for applying a TIG. This is determined by the surgeons’ preference. The same can be said for the sutures used.
The relocation and suture fixation of the medial crura onto the nasal septum is a static but reversible process. It can be gradually repeated during surgery until the desired projection and relocation is formed. The stable long-term results and minimum chance of sequelae are attributed to 1). preservation of the structural integrity of the cartilaginous nasal tip framework; and 2). the restoration and enhancement of tip support.
The increase in nasal skeleton support comes at the cost of a rigid nasal tip because the flexible membranous septum is sacrificed during the TIG procedure. This stiffness can sometimes lead to a static appearance in profile view during changes of facial expression such as laughing; it becomes even more apparent when the depressor nasi-muscle is divided. For some surgeons, this rigidity is sufficient reason not to perform TIG; however, in other surgeons experience the patient’s complaint about a stiff nasal tip, is outweighed by their major improvement in subjective body image.
In addition to TIG, incision and reduction manoeuvres such as a medial or lateral crural overlay are sometimes indicated. These manoeuvres mainly concerned cases with severe over projection of the nasal tip for which a setback of the medial crura leads to an unacceptable degree of tension in the lower lateral cartilages. The use of septal extension grafts in combination with TIG requires specific attention because these manoeuvres are complementary to the end result.
Conclusion
TIG is a reliable technique that can help deliver consistently good results in patients seeking aesthetic rhinoplasty. These patients tend to have a small additional functional improvement as well.
The tongue in groove technique provides a reliable and reproducible method to recreate nasal tip support mechanisms. This also allows the tip to be repositioned to provide adequate nasal tip projection. The additional surgical manoeuvres required are intricate but provide good tip support and a strong base for other techniques like suturing and tip grafting. If more tissue contracture is expected as in revision rhinoplasty and in patients with thick sebaceous skin it may be beneficial to increase tip projection more than required to compensate for the possible reduction. Even though with TIG there is a possibility for increased stiffness for the tip the predictability of tip position largely outweighs the risks.
Table 1: Tip supporting mechanisms4
| Major Attachment of medial crural footplate to the caudal border of the septum. Attachments of the alar cartilages to the upper lateral cartilages. Size, shape and resilience of the medial and lateral crurae. |
| Minor Anterior maxillary spine and soft tissue attachment of the medial crural feet. Membranous septum. Cartilagenous septal dorsum. The ligamentous attachment between both lower lateral cartilages over the septal angle. Sesamoid cartilages extending to the pyriform aperture. The attachment of skin and muscles to the lower lateral cartilages. |
Table 2: Overview of TIG literature findings based on full-text available articles in the English literature2
| TIG indication | Author (year) | Rhinoplasty approach and sutures | Article highlights |
| To set an appropriate alar–columellar relationship | Shah et al (2015)13 | External/resorbable | N = 20, morphometric 3D photoanalysis. Signifi- cant improvement of columellar show and nasal tip rotation over time. |
| Williams (2012)6 | Endonasal/PDS 4–0 | N = 49, empirical report. Corrects excess columel- lar show, adds to long-term support, and delivers slight increase of projection. Occasional columellar cellulitis treated with oral antibiotics. | |
| To set tip projection and rotation | Foda (2003)7 | External/chromic 4–0 | N = 143 droopy tip, photographical measure- ments. Significant increase in rotation, insignificant increase in projection. Long-lasting results. |
| Datema and Lohuis (2015)8 | External/vicryl 4–0 and nylon 5–0 | N = 22, overprojected tip, PROMs, and photo- graphical measurements. Long-lasting deprojec- tion and rotation. High patient satisfaction with occasional transient complaint of tip stiffness. | |
| Lohuis and Datema (2015)9 | External/vicryl 4–0 and nylon 5–0 | N = 110, functional and aesthetic PROMs. Long-lasting, good results reported by patients. | |
| To add or restore support to the nasal base and extension grafts | Guyuron and Varghai (2003)10 | External/nylon 5–0 or PDS 5–0 | N = 27, short noses. TIG facilitates stability of the septal extension graft between two extra-long spreader grafts. |
| Shah and Miller (2006)5 | Endonasal/chromic 4–0 or PDS 4–0 | Empirical report. TIG to compensate postoperative loss of projection and counterrotation in ade- quately projected or slightly overprojected noses. | |
| Toriumi (2006)11 | External/plain catgut 4–0 and nylon 5–0 | Empirical report on nasal tip contouring. TIG to stabilize the nasal base, with or without septal extension. | |
| Margulis and Harel (2007)12 | Endonasal/nylon 3–0 mattress for 1 mo | N = 23, ptotic tips. Horizontal septal extension strut (tongue) supported between medial crura (groove). 87% long-lasting results | |
| All of the above | Kridel et al (1999)1 | Endonasal and external/chromic or PDS | N = 287, excessive columellar show, droopy tip, caudal septal deviation, wide columella. 97% success rate |
Abbreviations: PDS, polydioxanone suture; PROMs, patient-reported outcome measures; TIG, tongue-in-groove.
References
- Kridel RW,Scott BA,Foda HM, The tongue-in-groove technique in septorhinoplasty. A 10-year experience. Archives of facial plastic surgery. 1999 Oct-Dec; [PubMed PMID: 10937111]
- Datema FR,Lohuis PJ, The Tongue-in-Groove Technique in Primary and Revision Rhinoplasty. Facial plastic surgery : FPS. 2016 Aug; [PubMed PMID: 27494586]
- Williams EF, Alar-columellar disharmony using the tongue-in-groove maneuver in primary endonasal rhinoplasty. Archives of facial plastic surgery. 2012 Jul-Aug; [PubMed PMID: 22801799]
- Dyer WK 2nd, Nasal tip support and its surgical modification. Facial plastic surgery clinics of North America. 2004 Feb; [PubMed PMID: 15062235]
- Petroff MA,McCollough EG,Hom D,Anderson JR, Nasal tip projection. Quantitative changes following rhinoplasty. Archives of otolaryngology–head [PubMed PMID: 1863446]
- Farrior EH, Dramatic refinement of the nasal tip. Otolaryngologic clinics of North America. 1999 Aug; [PubMed PMID: 10433659]
- GOLDMAN IB, The importance of the mesial crura in nasal-tip reconstruction. A.M.A. archives of otolaryngology. 1957 Feb; [PubMed PMID: 13393909]
- Peck GC, The onlay graft for nasal tip projection. Plastic and reconstructive surgery. 1983 Jan; [PubMed PMID: 6849020]
- Sheen JH, Achieving more nasal tip projection by the use of a small autogenous vomer or septal cartilage graft. A preliminary report. Plastic and reconstructive surgery. 1975 Jul; [PubMed PMID: 1144545]
- Anderson JR, New approach to rhinoplasty. A five-year reappraisal. Archives of otolaryngology (Chicago, Ill. : 1960). 1971 Mar; [PubMed PMID: 5542353]
- MILLARD DR, ADJUNCTS IN AUGMENTATION MENTOPLASTY AND CORRECTIVE RHINOPLASTY. Plastic and reconstructive surgery. 1965 Jul; [PubMed PMID: 14310546]
- Johnson CM Jr,Godin MS, The tension nose: open structure rhinoplasty approach. Plastic and reconstructive surgery. 1995 Jan; [PubMed PMID: 7809266]
- Gunter JP,Clark CP,Friedman RM, Internal stabilization of autogenous rib cartilage grafts in rhinoplasty: a barrier to cartilage warping. Plastic and reconstructive surgery. 1997 Jul; [PubMed PMID: 9207674]
- FRED GB, Excessive forward projection of the nasal tip in rhinoplasty. A.M.A. archives of otolaryngology. 1958 Nov; [PubMed PMID: 13582365]
- Tremp M,Haack S,Mijuskovic B,Haug M, Suture techniques and cartilage grafts in nasal tip surgery: An algorithm in primary and secondary rhinoplasty. Journal of plastic, reconstructive [PubMed PMID: 31668523]
- Foda HM, Management of the droopy tip: a comparison of three alar cartilage-modifying techniques. Plastic and reconstructive surgery. 2003 Oct; [PubMed PMID: 14504527]
- Foda HM,Kridel RW, Lateral crural steal and lateral crural overlay: an objective evaluation. Archives of otolaryngology–head [PubMed PMID: 10604416]
- Datema FR,Lohuis PJ, Tongue-in-Groove Setback of the Medial Crura to Control Nasal Tip Deprojection in Open Rhinoplasty. Aesthetic plastic surgery. 2015 Feb; [PubMed PMID: 25491013]
- Lohuis PJ,Datema FR, Patient satisfaction in Caucasian and Mediterranean open rhinoplasty using the tongue-in-groove technique: prospective statistical analysis of change in subjective body image in relation to nasal appearance following aesthetic rhinoplasty. The Laryngoscope. 2015 Apr; [PubMed PMID: 25389075]
- Kridel RWH,Delaney SW, Commentary on: Effects of the Tongue-in-Groove Maneuver on Nasal Tip Rotation. Aesthetic surgery journal. 2018 Sep 14; [PubMed PMID: 29912277]