Intro/Background:
Controlling the shape and position of the nasal tip has been described as the single greatest challenge in rhinoplasty. In his textbook, Surgical Anatomy of the Nose, Tardy states it is impossible to sculpt the nasal tip and predict healing without completely understanding the tip support mechanisms of the nose1. Whether performing an open or endonasal approach, major tip support structures such as the scroll ligament and medial crural attachments to the nasal septum are routinely violated by common rhinoplasty techniques. Because of this, reconstructing tip support is mandatory with different methods available to accomplish this goal. Unfortunately, surgeons have been frustrated by a lack of predictability in reconstructing tip support noting that “how it looks on the table” may not equal the final result months to years later. This humbling aspect of the procedure has pushed surgeons to look for improved methods of tip control and support to attain more predictable and long-lasting results. This chapter aims to describe the current evidence and common methods used to maintain tip support: the columellar strut, tongue-in-groove, and septal extension graft.
Methods for controlling tip support:
A discussion of tip dynamics is one of the most intricate discussions in rhinoplasty. Our aim is to focus on the important aspects of tip support described in the literature. Toriumi describes the importance of stabilizing the base of the nose with commonly used strategies: columellar strut graft (CS), the septal extension graft (SEG), and tongue-and-groove (TIG). These three methods are the most commonly used by surgeons to maintain tip or improve tip projection2. Tip grafts, such as the shield graft, can increase projection and tip definition. However, this is not a structural graft used in the prevention of post-operative tip ptosis. Therefore, these will be excluded from our discussion in this chapter. We aim to review the common methods of tip support mentioned above and expand upon their use in modern day practice.
Columellar Strut
The CS has been the workhorse of rhinoplasty surgeons to support and control the nasal tip during rhinoplasty for many years. It was first described by Eitner in 1932 as a means to support tip projection (nasal tip grafts) and later described as a free-floating cosmetic graft by Goldman. In brief, a small rectangular piece of rigid cartilage or bone approximately 8-12mm in length, 3-4mm wide, and 1-2mm thick is placed between the medial crura and secured with sutures. This graft can be placed during both open and endonasal procedures. For endonasal placement, a pocket is made between the medial crura via retrograde dissection and the graft and secured with sutures to the medial crura. During an open procedure, the surgeon has options of securing the graft to the surrounding tissues such as the caudal septum or the maxillary crest, but can opt to have a “free floating” strut as well. Achieving more tip projection is possible by advancing the medial crura on the strut and securing them at this more advanced point.
Caudal Septal Extension Graft:
The SEG was first described by Bryd in 1997 as a graft fixed to the caudal or dorsal septum and secured between both lower lateral cartilages. Byrd found that tip modification in rhinoplasty frequently disrupted medial crural attachments to the septum and thus destabilized the nasal tip. Patients with weakened cartilages were at especially high risk of post-operative tip collapse. His original paper noted loss of tip projection using CS but maintained or increased tip projection when using SEG’s3. The SEG was later popularized by Toriumi and others for use in aesthetic rhinoplasty as a stable way to control tip projection, rotation, and nasal length4. In brief, the SEG is a piece of cartilage that allows modification of both the anterior and posterior septal angle. This allows full control of the nasal tip position and columellar shape. The graft is secured to the native caudal septum providing the firm base for which the rest of the tip is constructed upon. Tailoring the graft and methods of fixation to the caudal septum will be further expanded upon later in this chapter.
Tongue-in-Groove:
The discussion of tip support would not be complete without mentioning the tongue-in-groove (TIG) technique first described by Rethi and then popularized by Kridel in 19995. This technique involves cephalloposterior displacement of the medial crura onto the caudal septum and uses the inherent strength of the septum as the building block for rigid tip support. Kridel discusses the effect the TIG has on columellar show, tip rotation/projection, columellar narrowing, and straightening of the caudal septum. His paper does not address tip support directly. Later papers by Dobratz and Akkus focus on the TIG for tip support and will be discussed in this chapter2. The SEG is similar to the TIG concept with both techniques using the strength of the caudal septum as the main anchor of tip support. However, securing the medial crura directly onto the caudal septum is a powerful maneuver and is at great risk of over-rotation4. It is in these instances where the SEG plays an important and complementary role to the TIG technique.
Tip support- the evidence
It is important to note that the tip support technique chosen in each case is influenced by many factors and not based on tip support alone. Each of the techniques below may be chosen for its overall effect on projection, rotation, and the columellar-labial angle relationship. For example, the CS may be used to stabilize weak or buckled medial crura. The SEG and TIG can both be used to rotate and project the tip but the SEG may be used to increase columellar show where the TIG may be used to decrease it. However, the specific question of which technique provides better long term tip support is an important one. Several articles have discussed these techniques and compare their outcomes.
Dobratz et al performed a study comparing tip support using the CS, TIG, SEG, and tip sutures in both clinical rhinoplasty patients and cadavers. The clinical portion of the paper was a retrospective review of forty patients and compared changes in nasal tip rotation using preoperative, short term post-operative (< 12 weeks), and long-term post-operative (> 52 weeks) time frames. Tip rotation was evaluated by two blinded facial plastic surgeons using lateral photographs. Their results showed no statistical difference between techniques when comparing short-term and long-term photographs2.
In the cadaver study, five fresh cadavers underwent the four tip support techniques described previously and the amount of resistance to posterior retropulsion of the nasal tip was measured. This was accomplished using a tensometer device which applied weight to the nasal tip in 5g increments. After each increase in weight, the amount of posterior displacement was measured. Their results show that the TIG and SEG provide more resistance than CS and tip sutures alone. This difference is likely from the TIG and SEG both using the septum as its anchor point. However, the clinical study did not show any difference between the four maneuvers. The authors believe this was a result of selection bias as the technique chosen was not randomly selected. Inherent anatomical differences in the pre-operative tip support may have influenced which technique was used and may explain why no difference was seen post-operatively.
Akkus et al compared the difference in tip support provided by CS and SEG in cosmetic rhinoplasty patients. They examined the differences in ratios of nasal projection to nasal length and columella labial angle values in 36 patients in the early (4-8 months) and late (16-24 months) post-operative periods. Both grafts achieved an increase in tip projection in the early post-operative period. In the late post-operative period, there was no significant difference between the grafts. However, the values in the SEG group were found to decrease less than the CS. Therefore, they conclude that while no statistical difference was found, patients at high risk of tip ptosis should undergo SEG over CS6.
Wilston et al assessed nasal tip resistance to compression in 6 fresh cadavers who underwent tip sutures, CS, and CSE grafts. Tip support following CSE was significantly better from all other methods resulting in a 66.7% increase in resistance compared to the pre-operative assessment. CS placement showed no change in resistance from pre-operative assessment. Tip sutures alone showed a decrease of 24.9% in resistance compared to pre-operative assessment7.
The data presented seems to suggest that using the septum is the best scaffold to support the nasal tip. If this is true, then one would hope these techniques would show long term stability of nasal rotation when they are used. Recently, Sawh-Martinez published a retrospective cohort study comparing 106 patients who received either CS (42%) or SEG (58%) to increase nasal projection8. Photographs were analyzed pre-operatively, 6 weeks post-operatively, and at least 12 months post-operatively. Analysis showed statistically significant greater maintenance of tip rotation over time with SEG vs. CS (-1.01% change vs. -5.08%). Tip projection, nasal length and Goode’s ratio all decreased for both groups over time, but were not statistically significant. Similarly, Antunes and Quatela published on a series of 17 patients who underwent the TIG maneuver and assessed nasal tip rotation pre-operatively, immediately post-operatively, and 1 year post-operatively9. They found the nasal tip dropped an average of 7.9 degrees, which was statistically significant. These studies both conclude that even when using the septum as a base of support (SEG/TIG), patients lose tip support and rotation post-operatively in a significant way. This post-operative drop in tip projection can be clinically relevant and is a main factor for surgeons who have gone away from CS in lieu of SEG’s. The evidence supports the concept that SEG’s are beneficial in the amount of tip support provided versus other standard techniques. Because this technique has the most technical variations, we will expand on SEG’s specifically for the rest of the chapter.
Technical Considerations of SEG’s
Indications:
SEG’s are indicated when considerable changes to the nasal tip are required. As discussed previously, the SEG allows control of multiple variables of the tip and is especially useful when attempting to lengthen the nose and preserve rotation (Wong). In patients with long caudal septums, the TIG technique is a reliable option, however routine use risks over-rotating the nose. In these scenarios the SEG is useful and allows tip modification with preservation of rotation. Another indication for use is when rigid tip support is desired by the surgeon. Patients at high risk of tip ptosis (weak or short medial crura) or scar contracture (revision rhinoplasty) are good candidates for SEG use.
Material for SEGs:
Grafts may be fashioned from septal cartilage, conchal cartilage, or costal cartilage. Descriptions of SEG’s in the literature require the graft to be both strong and straight, making septal cartilage the ideal substrate. Auricular cartilage lacks these characteristics and is less preferred. In revision rhinoplasty where septal cartilage may be wanting, costal cartilage is often needed.
Classification of SEG:
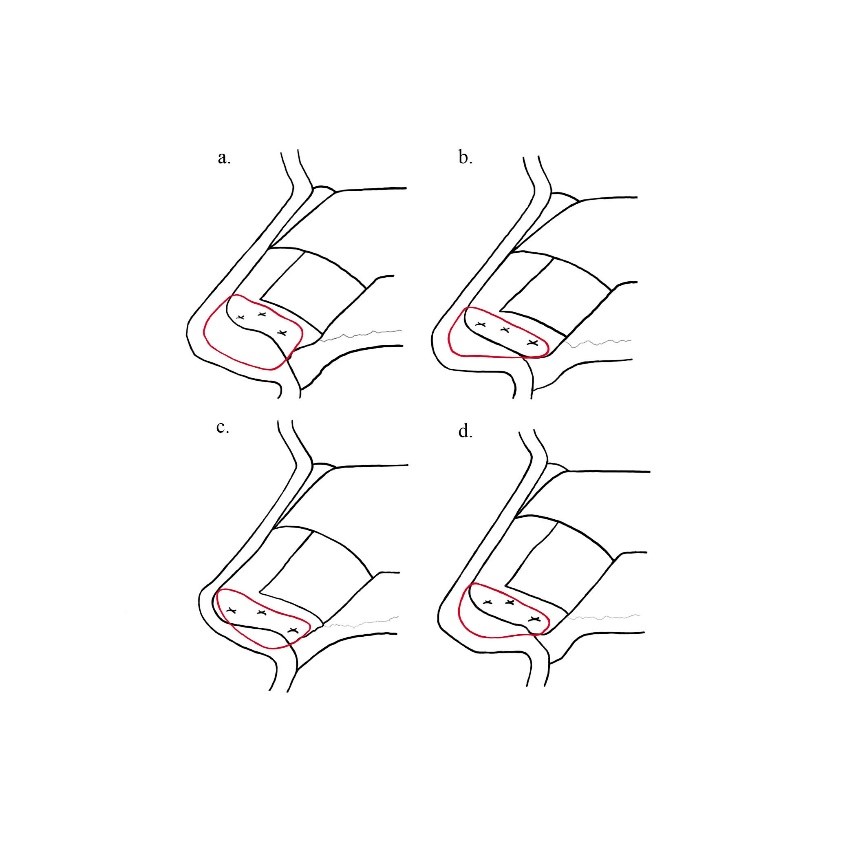
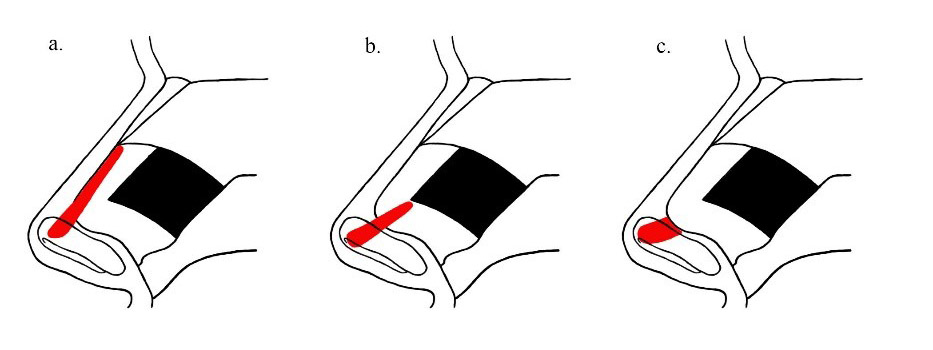
Type 1: Paired Spreader Grafts
Bilateral spreader grafts are fashioned and placed between the septum and upper lateral cartilage bilaterally. The grafts are long enough to extend into the space between the medial crura. The tip lobule complex should be fixed to these grafts.
Type 2: Paired Batten Grafts
These are fixed at the corner of the L-strut after cartilage graft harvest has been completed. They should be placed where the dorsal and caudal septa meet. This graft is preferred when no middle vault reconstruction is desired or needed and thus Type 1 spreader grafts are not an option.
Type 3: Direct Extension
This graft is affixed directly to the anterior septal angle via a figure eight clocking stitch. This graft is placed either end to end or on one side of the septum. The end to end fixation is not as rigid as the other two options, risking tip asymmetry when fixing the tip lobule complex to the extension graft. It is used when insufficient cartilage is obtained as it uses the least amount of graft material. Toriumi has described using paired extended spreader grafts to fix a direct extension SEG as well1.
Securing SEGs
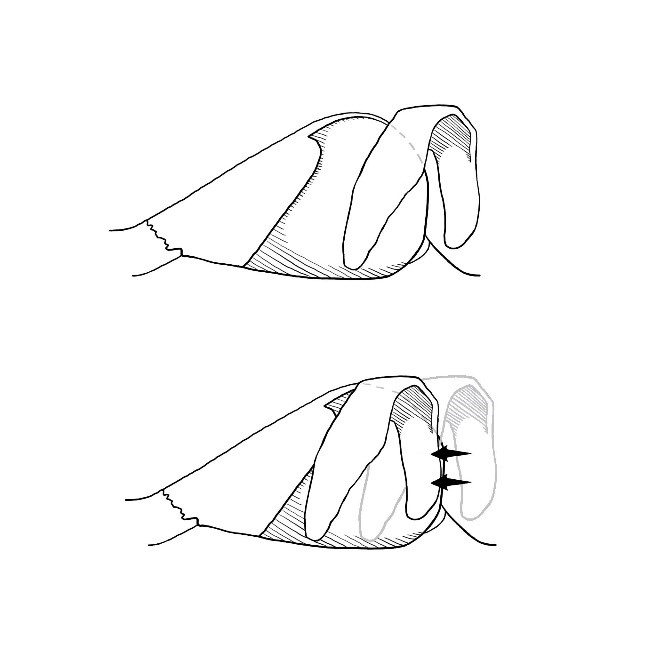
The basis of using SEG’s for tip support is its fixation to the caudal septum. The saying “where the caudal septum goes, the tip follows” emphasizes the need for both a strong and straight piece of material which is firmly affixed to the native septum. New techniques have improved on Byrd’s original description and show that with the direct extension method, a single vertical figure-of-eight locking suture is the most secure fixation. Han et al applied shearing, buckling, and tensile forces to SEG’s and compared the strength of two simple interrupted sutures, two horizontal figure eight locking sutures, and one vertical figure-of-eight locking suture. They found one vertical figure-of-eight suture was the strongest method to secure the graft. The overlapping method has been shown to be more stable than direct extension when overlap of at least 4mm occurs, but this does require a larger SEG (more cartilage)10. The overlapping method also requires the graft to sit on one side of the septum potentially complicating absolute midline placement of the graft. Toriumi and others describe using opposing curves of the SEG and caudal septum to one’s advantage to have the SEG sit in the midline. Tebbets described his dovetail junction modification to solve this problem with the SEG placed into a groove carved in the caudal edge of the septum allowing it to sit perfectly in the midline. However, this technique is technically challenging given the thin nature of the caudal septum. Whichever method the surgeon chooses for graft fixation, it must provide a strong and stable base of support for the nasal tip and it must lie in the midline or risk deviations and asymmetries of the tip.
Tailoring SEG’s:
The SEG has a great deal of versatility to modify tip position. Depending on the shape of the graft, it can alter the nasolabial angle, nasal length, tip rotation, tip projection, and columella-ala relationship. For a ptotic tip with an acute nasolabial angle, a longer inferior portion of the graft is tailored to blunt the acute angle and support the tip. For an over-rotated nose with short nasal length, a longer superior portion is tailored to counter rotate the tip and lengthen the nose. The SEG should be placed so that approximately half its length it is projecting into the interdormal area above the anterior septal angle. Initially it should be longer than necessary and once the nasal skin is redraped, the SEG can methodically be trimmed until the desired projection is achieved. Next the domal parts of the medial crura are secured to the SEG. The location of this suture is similar to an inter-dormal suture. If any graft remains projecting above the domes it is trimmed and the domes can be further refined with standard rhinoplasty tip suturing.
Disadvantages/Complications:
A disadvantage of the SEG compared to tip sutures or columellar struts, is tip stiffness. While this is a benefit to the surgeon worried about tip ptosis, patients may complain about this tip rigidity. The SEG can also cause nasal obstruction by narrowing the external nasal valve if it is too wide and/or secured in an overlapping fashion. It is critical to evaluate the external valve pre-operatively and modifications of the graft may be necessary if intraoperative assessment shows the SEG impacting its function. Finally, SEG’s require more cartilage and in patients with limited septal cartilage or in revision rhinoplasty cases, this may require auricular or costal cartilage harvest. This addition of a donor site and its possible morbidity is another disadvantage to SEG use.
Summary:
Controlling the nasal tip is perhaps the most challenging aspect of rhinoplasty. Options for providing a stable base for the tip include the columellar strut, tongue-in-groove, and septal extension graft techniques. Methods that use the septum (SEG/TIG) appear to have increased resistance to healing forces that lead to tip ptosis over time, however they are not completely resistant. One powerful method of providing tip support is the septal extension graft. This graft has the ability to control the nasolabial angle, nasal length, tip rotation, tip projection, and columella-ala relationship at the same time. Thus, it is an important technique for the modern rhinoplasty surgeon looking to modify multiple factors of the nasal tip while providing a strong base of support.
References:
1. Toriumi DM1, Checcone MA. New concepts in nasal tip contouring. Facial Plast Surg Clin North Am. 2009 Feb;17(1):55-90
2. Dobratz EJ, Tran V, Hilger PA. Comparison of techniques used to support the nasal tip and their long-term effects on tip position. Arch Facial Plast Surg. 2010 May-Jun;12(3):172-9.
3. Byrd HS, Andochick S, Copit S, Walton KG. Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg 1997;100 (4) 999- 1010
4. Chiu-Collins L.L., Furze A.D., Wong B.J.F. (2013) Caudal Septal Extension Grafts. In: Shiffman M., Di Giuseppe A. (eds) Advanced Aesthetic Rhinoplasty. Springer, Berlin, Heidelberg
5. Kridel RW, Scott BA, Foda HM. The tongue-in-groove technique in septorhinoplasty: a 10-year experience. Arch Facial Plast Surg 1999;1 (4) 246- 258
6. Akkus AM, Eryilmaz E, Guneren E. Comparison of the effects of columellar strut and septal extension grafts for tip support in rhinoplasty. Aesthetic Plast Surg. 2013 Aug;37(4):666-73.
7. Willson TJ1, Swiss T2, Barrera JE3. Quantifying Changes in Nasal Tip Support. JAMA Facial Plast Surg. 2015 Nov-Dec;17(6):428-32.
8. Sawh-Martinez R1, Perkins K, Madari S, Steinbacher D. Control of Nasal Tip Position: Quantitative Assessment of Columellar Strut vs Caudal Septal Extension Graft. Plast Reconstr Surg. 2019 Jul 30.
9. Antunes MB, Quatela VC. Effects of the Tongue-in-Groove Maneuver on Nasal Tip Rotation.
Aesthet Surg J. 2018 Sep 14;38(10):1065-1073. doi: 10.1093/asj/sjy078.
10. Han K, Jin HS, Choi TH, et al. A biomechanical comparison of vertical figure-of-
eight locking suture for septal extension grafts. J Plast Reconstr Aesthet Surg. 2010;63:265–269.