Introduction
Ideal positioning of the nasal tip is a very important element to a successful rhinoplasty. Tip projection, rotation, angulation of the infratip lobule, and the columellar-labial junction are controlled by the surgeon. There are numerous methods described in the literature regarding tip stabilization[1][2][3][4]. These include but are not limited to, medial crura binding suture, columellar struts, caudal septal extension grafts, tongue-in-groove suturing technique, and septo-columellar sutures (SCS). These are all valid techniques and each have their indications depending on the situation at hand. Regardless of the method chosen, it is the details of how it is carried out that will determine a successful outcome. This chapter will specifically focus on the fine points of suturing the columellar complex to the caudal septum for determining tip position and stabilization.
Tip support
It has long been understood and accepted that wound contracture will affect the alar cartilages even if they have only been minimally modified[5] . Current rhinoplasty techniques routinely involve disrupting the relationships between the medial crura, domes, and the relationship of these structures to the caudal septum. In particular, maneuvers that divide between the crura to approach the septum render the tip with compromised support. At the completion of any rhinoplasty, the tip must be situated in the ideal position and stabilized. Just relying on the inherent stiffness of the cartilages themselves, or even with the addition of a strut bound between them leaves a significant amount of unpredictability as to where things will end up after healing takes place. Thus, securing the tip somehow to the most stable fixture of the nose, the septum, has become not only commonplace but essential.
Septo-Columellar Suture versus Tongue-In-Groove
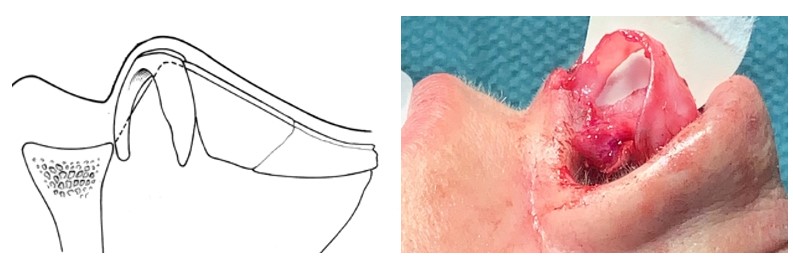
The SCS is essentially a loop suture binding the columella to the caudal septum[6]. Of note, this is not a tongue-in-groove (TIG) suture where the medial crura straddles the end of the septum (Figure 1). The TIG technique results in shortening of the nose, flattening of the infratip and a stiffer nasal tip over the long term. In order to prevent shortening the nose too much when using a TIG, a caudal septal extension graft can be secured first, however this then creates other technical challenges and potential pitfalls.
Anatomic Rationale
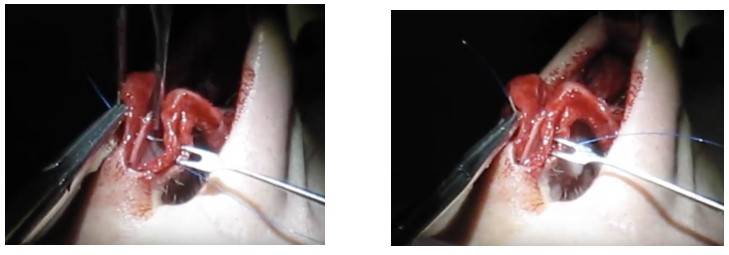
Although medial crura have great variability with respect to their shape and size, they are fairly consistent in the way they relate to the caudal septum. Posteriorly, the cephalic ends of the medial crural footplates approximate and usually overlap the underlying caudal septum. Anteriorly the medial crura diverge from the caudal septum resulting in a gap between the two. It is this relationship that allows for flexibility when we apply SCS and which forms the basis for how suture placement can create the desired effects. The anchoring point for all sutures is the caudal septum and the point where the columella is engaged by the suture will be directed to that fixed spot (Figure 2 and Video1).
SCS Suturing Technique
With an endonasal approach the medial crura are usually separated from the septum via a transfixion incision, but a hemitransfixion incision can also be used. With the open technique, no mucosal incisions are necessary as the caudal septum is approached by dissecting between the medial crura. To obtain a better understanding of the relationship between the medial crura and caudal septum, the vestibular skin is freed off the medial crura (Figure 3). Oftentimes, the vestibular skin is freed entirely, but this is a matter of choice. The senior author prefers to bury all sutures, but if a surgeon is comfortable leaving sutures exposed then this dissection can be omitted. However, the senior author has found that by freeing the vestibular skin, he is better able to align the skin edges during closure of the transcolumellar incision. Once the cartilages are exposed, binding the columella (i.e. paired medial crura with or without a strut) to the caudal septum and the relationship between them will determine tip position.
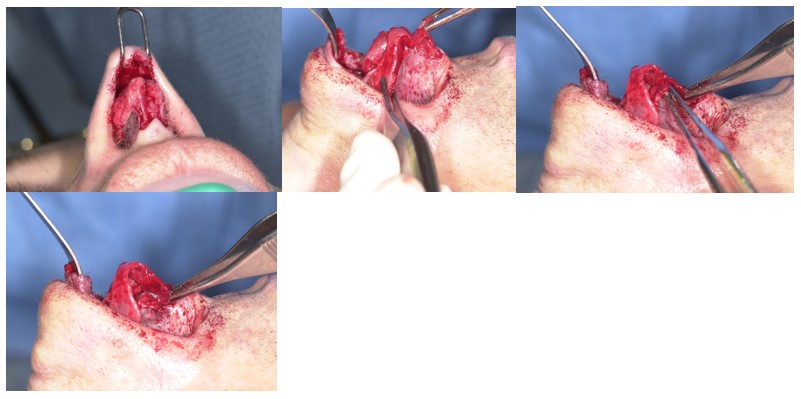
Intraoperative photo depicting freed vestibular skin from the undersurface of the entire LLC.
The columellar complex: Strut or no strut.
Prior to securing the columella to the caudal septum it must be determined whether to place a strut between the medial crura or simply combine them together as is. A strut is applied when the medial crura are particularly thin or weak and also when it is necessary to add a small amount of length at the columella and infratip. In order to assess the impact columellar struts have on columellar show, the senior author conducted a retrospective chart review over a 5-year span. He found that when columellar struts were used, they increased columellar show at the subnasale and increased the width of the columella. However, if a columellar strut is used with a septocolumellar suture, this combination negates the change in columellar show (Frankel, unpublished data 2012).
The senior author also feels a strut adds stability and minimizes the chance for the columella to twist. When it’s desired to thin out the columella or when there is limited cartilage available then the bound crura alone can suffice. It’s important to note that binding the medial crural feet to one another posteriorly causes them to move caudally in front of the anterior nasal spine. This can create more columella show and a more obtuse columellar-labial angle which might be detrimental or beneficial depending on the goals (Video 2).
Nuances of Septo-Columellar Suturing Technique (Video 3)
Increasing tip projection
If the goal is to solely increase projection without rotation then the columella must be engaged at a position where it is in the same plane as the leading edge of the septum (where it intersects with the edge). This point is usually located closer to the anterior nasal spine. The septum is then engaged with the suture at a point located more anteriorly. The degree of projection will be determined by how far forward the septum is engaged (Figure 4a,b).

Intraoperative photo demonstrating the relationship of the medial crus to the caudal septum

Increasing projection without rotation – The medial crura (black dot) always move towards the fixed caudal septum (blue dot)
If a significant amount of tension is required, then a 5-0 Prolene (Ethicon Suture) is employed. Although permanent sutures carry a risk of infection, they do provide long term support to resist wound contraction and loss of tip projection. To counter any torque attributable to the first suture, a second one is thrown with the knot on the other side and this one is almost always a 5-0 polydioxanone (Ethicon Suture, PDS)(Video 4).
Decreasing tip projection
For this goal, the columella is engaged at a point anterior to its counterpart along the caudal septum, so when the suture is tied down, the tip is deprojected. Non-absorbable sutures are adequate for this since there is little tension when deprojecting the nose. Occasionally, the medial crura will need to be trimmed to prevent bunching or narrowing of the vestibule. While it is common to decrease projection using SCS, it is impossible to use these techniques to counter rotate the tip, and for that effect a caudal septal extension graft must be used (Figure 4c).

Deprojection
Rotation of the tip complex
The medial crura are curved structures leading in front of the septum anteriorly and overlapping it posteriorly. When a SCS is used to close the gap between the paired medial crura and caudal septum, shortening or rotation occurs. Depending on the placement of the sutures, this can solely rotate the tip or simultaneously rotate and increase projection.
If the desire is to rotate only – the columella is engaged where there is a space between it and the septum. The septum is then grasped immediately across the gap to bind the two structures. The greater the gap, the greater degree of rotation and this is usually the case the further anteriorly the sutures are placed. By bringing the columella up to and abutting the caudal septum more posteriorly (where there is less of a gap) you more conservatively shorten and rotate the nose (Figure 4d).

Rotation
If the desire is to rotate the tip and increase tip projection – the columella should be grasped posteriorly and secured to the septum further anteriorly to lock in the projection. A second suture is then used to close the gap between the columella and septum anteriorly which will create the desired rotation. Although a single suture placed properly can create both effects, two sutures might allow for greater control. The first suture is used to lock in the projection and the second to rotate that part of the tip complex above where the first suture was tied down. (Video 5 and Figure 4e).

Increasing projection with rotation (black dot anteriorly on medial crus, move blue dot toward anterior septal angle)
Summary
Although the use of septocolumellar sutures is a well established method of stabilizing the nasal tip, there has been little described in the literature regarding how to place them to achieve various desired outcomes. As with many things, the devil is in the details and in this chapter we outlined the anatomic basis for achieving different effects by placing the sutures in specific manners. The methods described herein are meant as a general guide and the surgeon should always analyze the tip after each suture is thrown and remove and replace them when necessary. Once the surgeon becomes familiar with these concepts they will have a greater mastery over the aesthetics of the nasal tip.
References
- Gandy JR, Manuel CT, Leary RP, Wong BJ. Quantifying Optimal Columellar Strut Dimensions for Nasal Tip Stabilization After Rhinoplasty via Finite Element Analysis. JAMA Facial Plastic Surgery. 2016 May 1; 18(3):194-200
- Kridel RWH, Scott BA, Foda HM. The Tongue-in-Groove Technique in Septorhinoplasty. A 10-year experience. Arch Facial Plastic Surg. 1999 Oct-Dec;1)4):246-56; discussion 257-8
- Toriumi DM. Nasal Tip Contouring: Anatomic Basis for Management. Facial Plastic Surgery and Aesthetic Medicine. 2020 February.
- Toriumi DM. Caudal septal extension graft for correction of the retracted columella. Op Tech Otol Head Neck Surg. 1995;6(4):311–318
- Park SS. Fundamental Principles in Aesthetic Rhinoplasty. Clin Exp Otorhinolaryngol. 2011 Jun; 4(2):55-66
- Tezel E, Numanoglu A. Septocolumellar Suture in Closed Rhinoplasty. Ann Plast Surg. 2007;59:268-272