In this chapter we will comment on the major sutures performed to achieve a proper nasal tip definition.
Transdomal suture
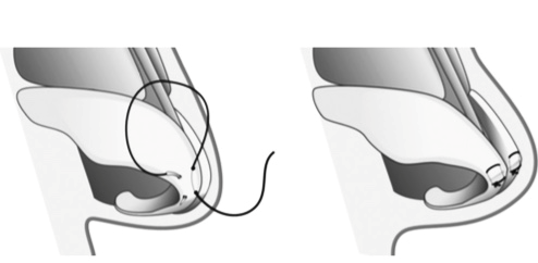
Transdomal sutures (TDS) are used to increase tip projection, narrow the distance between the domes and helps to form the tip double break and provide a better tip-columella relation.
The transdomal sutures are effective in flatening the lateral crura, shrink bulbous nasal tip due to horizontalization, reduction of the lobe size, reduced angle between the superior and lobular segments of the two medial crura
The sultures are usually positioned from 2 to 3 mm in both sides of the tip definition point. They are inserted into the cartilage horizontally . The knots are tied medially between the crura.
The results are: increased projection of the tip and depending on the position of the suture, we can observe a cephalic or caudal rotation of the lateral crura.
Interdomal suture
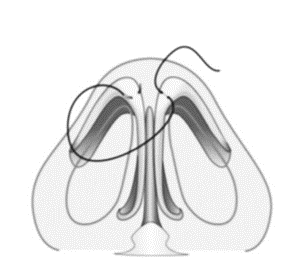
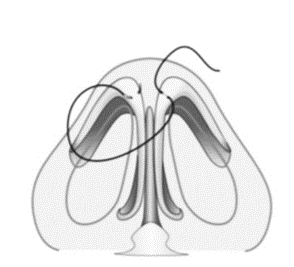
The interdomal suture is performed on the lower lateral cartilage dome. Its tightening must be gradual and progressive to permit adjustments . Performing the interdomal suture at the end of the surgery prevents excessive manipulation of the nose tip and possible enlargement of the interdomal distance.
Interdomal suture provides stabilization, tip rotation, narrowing and definition of the domus, interdomal width and tip equalization. Suturing is done at a level 3-4 mm posterior to the true domus and preserves the normal separation between the domes. A single loop suture is performed from the most anterior portion of the domus to the contralateral domus.
The interdomal suture approximates the domus and allows to equalize asymmetries between the domus. As the suture is fixed, the domus is approximated, which narrows the tip and decreases the width of the lobe. In general, a broader tip in male and thinner female patients can be controlled by interdomal and transdomal sutures.
Lateral Crural matters Suture
The control of nasal cartilage curvature is one of the dilemmas faced in the field of plastic surgery. Gruber proposed a suture technique that aims to correct an unwanted convexity in the lower lateral cartilages. In these cases, to correct the bulging of the masal tip, if the transdomal sutures are not sufficient, horizontal mattress sutures in the lateral crura can be used to rectify the cartilages to better define the tip. In this technique, the suture alters the original shape of the cartilage, individually, based on the tension exerted by the suture. It begins by infiltrating anesthetic solution at the lower edge of the lower lateral crura in order to distance the cartilage from the skin of the nasal vestibule. The lateral crus is fixed with Adson-Brown forceps, at the apex of the convexity, and a PDS 5-0 wire is inserted. The first pass of the needle is performed from the caudal to cephalic border (3mm), transversely along the long axis of the lateral crus; the second pass is made 6 to 8 mm after the first, this time from cephalic to caudal. A slip knot is provided to adjust the tension of the suture until the convexity is corrected. Note that the knot ends near the caudal edge of the lateral crus, where unwanted exposure is less likely to occur. If the convexity is not fully corrected, a second horizontal suture of the mattress (and even a third, if necessary) can be performed adjacent and posterior to the anterior suture. An additional advantage of this suture technique is the simultaneous improvement of the function of the external nasal valve, since the tension exerted on the posterior side of the lateral crus becomes more lateralized and stable. Thus, theoretically, the external nasal valve is slightly opened and stabilized.
Septal-columellar suture
The septal-columellar suture aims to fix the inferior lateral cartilages to the caudal septum, contributing to projection, rotation and stabilization of the nasal tip. The first pass of the needle is made between the middle crura, there is a lot of fibrous tissue in this space, then through the septum at the anterior septal angle, and finally the needle is passed back through the middle crura1. More recently, a double pass in the septal angle has been advocated for better suture stabilization. As the knot is slowly tightened, it pulls the lower lateral cartilages toward the caudal septum, correcting any existing hanging columella and also providing a small amount of tip projection.
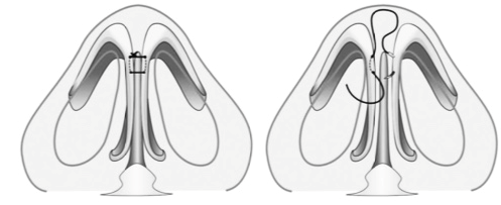
Intercrural suture
Intercrural suture is used to reduce the width of the cartilages in the middle crura. A PDS (5-0) is passed on the inner side of the middle crura (posterior to anterior) on one side and then on the contralateral side. The knot is located between the middle cruras. It is important to note that the knot should not exert too much tension, due to the risk of excessively narrowing the normal width of the middle crura.
A 36 year old female patient with a major complaint of nasal tip ptosis came to our service for rhinoplasty.We opted for open aproach, structuring the nasal tip with strutgraft and correcting the convexity of lower alar cartilages with tip sutures, Inter and transdomal Suture, Lateral Crural Mattress Suture, Medial Crural Fixation Suture. We can see the result of the surgery in the photos below and the intraoperative video.



REFERENCES
Gruber RP, Weintraub J, and Pomerantz J. Suture techniques for the nasal tip. Aesthetic Surg J 28:92–100, 2008.
C¸ akmak O¨ , and Akkuzu G. Primary tip rhinoplasty and suture techniques. Available online at https://www.rhinoplastyarchive.com/articles/primary-tip-rhinoplasty-and-suture-techniques; accessed January 7, 2015.
Guyuron B, and Behmand RA. Nasal tip sutures part II: The interplays. Plast Reconstr Surg 112:1130–1145; discussion 1146–1149, 2003
Toriumi DM. New concepts in nasal tip contouring. Arch Facial Plast Surg 8:156–185, 2006.
Tardy ME Jr, Patt BS, and Walter MA. Transdomal suture refinement of the nasal tip: Long-term outcomes. Facial Plast Surg 9:275–284, 1993.
Daniel RK. Tip. In: Rhinoplasty: An Atlas of Surgical Techniques. New York: Springer-Verlag, 59–139, 2002.
Toriumi DM, and Checcone MA. New concepts in nasal tip contouring. Facial Plast Surg Clin North Am 17:55–90, vi, 2009
Gruber RP, Nahai F, Bogdan MA e Friedman GD: Alterando a convexidade e concavidade de cartilagens nasais e enxertos de cartilagem com suturas horizontais de colchão: Parte II. Resultados clínicos. Plast Reconstr Surg 2005; 15: pp. 595-606.
Gruber RP: Discussão sobre “A ponta nasal quadrada: Classificação e tratamento com base na sutura da cartilagem alar” por Rohrich, RJ e Adams, WP, Jr. Plast Reconstr Surg 2001; 107: pp. 1866-1868
Cingi, C., Muluk, NB, Ulusoy, S., Söken, H., Altintoprak, N., Şahin, E., & Ada, S. (2015). Suturas nas Pontas Nasais: Técnicas e Indicações. American Journal of Rhinology & Allergy, 29 (6), e205-e211. https://doi.org/10.2500/ajra.2015.29.4236
Ronald P. Gruber, Jennifer Weintraub, Jason Pomerantz, Técnicas de sutura para a ponta nasal, Aesthetic Surgery Journal, Volume 28, Edição 1, janeiro de 2008, páginas 92-100, https://doi.org/10.1016/j.asj. 2007.10.004.
Ronald P. Gruber, Jennifer Weintraub, Jason Pomerantz, Técnicas de sutura para a ponta nasal, Aesthetic Surgery Journal, Volume 28, Edição 1, janeiro de 2008, páginas 92–100, https://doi.org/10.1016/j.asj. 2007.10.004.
Ronald P. Gruber, Simeon H. Wall, Jr., David L. Kaufman, David M. Kahn. Secondary rhinoplasty. Plastic Surgery E-Book: Volume 1 Principles, 2017, chapter 21.