Abstract
The current ideal nose is straight with a well-defined projected tip, covered with thin skin under which the osteocartilaginous support protrudes giving an impression of angularity. The radix should be located at the level of the upper edge of tarsal cartilage of the upper eyelid and the nasolabial angle should be between 90°–100°.
To achieve this ideal goal in a Hispanic nose it is necessary to modify the dorsum, the tip projection, the nasolabial angle, and the alar base, and to apply the structural concept of rhinoplasty for tip surgery.
Introduction
Hispanic people are a mixture of European settlers, mostly Spanish, and indigenous populations. In ethnology, these Europeans are commonly referred to as Caucasians and are considered Indo-Europeans and Native Americans descendants of the Mongolia tribes that migrated from northeast Asia.
The features of the “Hispanic face” vary according to the percentage of particular ethnic features in the individual. Some physical characteristics, however, are common to these people. The facial skeleton is characterized by a large bizygomatic diameter resulting in prominent cheek bones. Wide bigonial diameter may also be present. Prominence of the dental arches is a common trait. The mouth is projected anteriorly, resulting in an acute columellar-labial angle. The epicanthal fold is present in many cases.
The nose is relatively small with moderately thick skin. The skin thickness is related to the presence of a thin layer of subcutaneous fat, not to an excess of sebaceous glands, as is common in other races. The dorsum is convex with a minimal hump. There is no marked prominence of the nasal bones; the convexity is mainly related to the under-projection of the caudal half of the nose and a low nasion.
The tip is poorly defined and the columella is short because the cartilaginous arches are small and thin.
The nasolabial angle is acute (from 65° to 85°), partly because of the position of the nasal tip, but primarily due to the position of the upper lip projected by the protrusive dental arch. This also gives a false impression of a receding nasal spine.
The nostril base may occasionally be wide. In most cases this impression of broadness is produced by the lack of tip projection, that is, the relation between the width and the height of the triangle formed by the nostrils and the nasal tip.
The chin may be slightly receding when the lower third of the face is examined cephalometrically. The pogonion is often located in an ideal position but appears to be retruded because of the prominent dental arches.
The Dorsum
The slight dorsal convexity usually present in the hispanic nose should not necessarily be considered as an osteocartilaginous hump. In some cases the convexity can be corrected with a combination of tip augmentation and minimal dorsal resection. The convexity may be more evident when the nasion is low (that is, the lowest point on the frontonasal groove), requiring augmentation of the radix also.
The nose in this ethnic group is relatively small in relation to the face, sometimes requiring a complete dorsal augmentation. In the full-face view the nasal pyramid appears broad. Once the dorsum is augmented, the excessive width of the bony skeleton is no longer evident, so lateral osteotomies are not always necessary. In more conventional cases only a discrete resection of the osteocartilaginous dorsum is required.
The Tip
Most hispanic noses have limited tip projection because the medial crura of the alar cartilages are short and thin, corresponding to a short columella. The lateral crura are also narrow and thin. The relatively thick skin prevalent in this population has a layer of subcutaneous fat contributing to a lack of definition of the tip area.
The Nasolabial Angle
As mentioned above, the acute nasolabial angle of the hispanic nose results from the combination of the shape and position of the the alar cartilages, mainly the short medial crura and the position of the upper tip supported by the protruding alveolar ridge of the maxilla. The nasal spine appears receding.
Alar Base
The width of the alar base should be approximately the same as the intercanthal distance. The base is considered wide when it extends more than 2mm beyond a vertical line drawn from the medial canthus. Some hispanic noses present with a broad nostril base. In others the impression of width is produced by the limited tip protrusion. When the tip is augmented the problem is corrected. In others it is necessary to do a Weir resection of the nostril base.
Structural concept for the hispanic nasal tip
Structural rhinoplasty ensures an aesthetic and functional result that will last throughout life. The preservation and anatomization of structures is fundamental in these surgical techniques. It is important to understand that not all cases should apply structural grafts; it is important to make an accurate pre-surgical diagnosis.
Structural rhinoplasty is more of a concept than a technique and it is based on the ideology of preserving and anatomizing the existing structures of the nose and sometimes reconstructs what has already been damaged by a prior surgery or trauma. Over the years we have realized that long term results can be catastrophic when we resect excessively.
One of the most important issues in performing this procedure is to understand what we want to achieve with structural grafts, as well as make an accurate diagnostic of the anatomy of each nose.
Measurements are another basic aspect for rhinoplasty and for this three instruments in particular are used
- the projectometer serves to objectively quantify the projection, in addition to the height of the dorsum and radix (Image 1).

- The caliper helps to measure both grafts and nasal structures.
- The digital goniometer is used to measure angles and is indispensable for objectively measuring the positions of the lateral crural. (Image 2).

Surgical Approaches
The most commonly used surgical approach is the external one since the visual field and precision, in terms of the placement of grafts and their symmetry, are better achieved with this approach than with an endonasal surgical approach. However, an endonasal surgical approach is appropriate in some cases.
In the external surgical approach it is preferable to first make incisions along the lateral crural and then towards the middle crural in the nasal vestibule. Next, (with cutting dissection made) dissecting with converse scissors, the lateral cruras are exposed, the domes are dissected and the columellar skin of the middle crural. The most common columellar incision is an inverted V type and it is located at the junction of the middle and lower third of the columellar in most cases, that is, unless the patient requires a significant increase or reduction in tip projection. At the time of making the incision, the scissors are interposed between the skin and the middle crural to protect them and the skin is cut with a scalpel blade 11. Subsequently, the Pitangui ligament is identified and dissected in its insertion to the skin of the supratip to avoid the formation of a soft pollybeak deformity and to be able to perform a soft tissue graft type PAT. Dissection is then continued in the usual way towards the rest of the tip, and the dorsum if necessary. When closing the columellar incision it is important to use a deep stitch with 5-0 chromatic catgut to reduce tension and on the skin 3 vertical mattress type stitches with 7-0 nylon for the eversion of the edges and the rest of the stitches with 6-0 fast absorption gut.
Grafts
The use of grafts is fundamental to this procedure and in most cases cartilage is used. However, sometimes bone can be utilised, a good option are perpendicular sheet fragments of ethmoid.
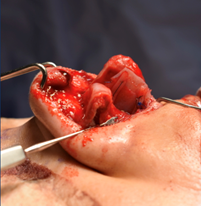
1.-Septal cartilage
The site for preference grafting is obviously the nasal septum due to accessibility and the firmness and shape of the quadrangular cartilage. However, the ethnic characteristics of Hispanic noses do not often allow for the extraction of sufficient cartilage. Further, many of the cases are revision surgeries and the remaining septal cartilage is scarce. It is important to remember that it is vital to maintain a septal structural framework that respects 1.5cm to 1cm of our L strut. We respect 1.5cm of dorsal septum and 1cm of caudal septum and septal work we do it after resection of the nasal dorsum. (Image 3).
2.- Auricular cartilage
Auricular cartilage is another site that can be used for grafts. The main limitation is its lack of rigidity. In its favor is easy accessibility. It is mainly used to make radix grafts, separating grafts in the cartilaginous vault, and septal extension grafts. The approach of choice for resection is anterior and the cymba shell is taken.
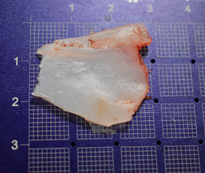
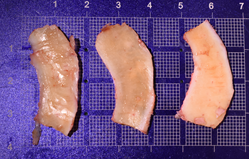
3.- Costal cartilage
The costal cartilage is an excellent option for structural rhinoplasty. Significant amounts of it can be obtained and it can be sculpted into various sizes and shapes; the rigidity of the cartilage is excellent. The main limitations are accessibility, in that, it is necessary to perform a more invasive procedure with greater risk, the inability of the surgeon to perform it due to lack of training, and the patient’s resistance to the procedure. However, in our experience, when the surgical options and procedure are fully explained to the patient, there is little resistance to the use of the costal graft. Another constraint is the tendency of the cartilage to bend but this can be predicted and prevented with various techniques.(Image 4)
For grafting, the fifth right rib is preferred in women. A 2.5cm incision is placed 1cm above the submammary groove medial to the areola. In men, the sixth and seventh ribs, which are easier to access, can be used.
Types of grafts
Depending on the requirements of each patient, the following structural grafts are used: (They will be described later in the chapter).
- Septal extension graft
- Columellar Strut
- Strut of lateral crural (with or without replacement of the crural)
- Graft of the alar edge
- Graft in shield
1. Septal extension graft
This is the most structural graft of all since it involves projection, rotation and tip support. Described by Byrd, who mentions several ways of fixation being called the best end to end. The fixation is performed using the technique described by Toriumi utilising two thin sheets of cartilage on each side and 5-0 permanent suture material.

Another way to perform the septal extension graft when the septal cartilage is insufficient is with folded auricular cartilage. Here, the septal caudal edge between both sides is set with permanent suture 5-0.
It is imperative to always set the average cruras to the graft with the “tongue in groove” technique.
The septal extension graft is a very powerful tool in the management of the nasal tip but it can also result in complications, of which the most frequent ones are mentioned below.
- Hard Pollybeak, which occurs when the septum is too short and the graft is taller than the septum.
- Hanging columella, which happens when the septal extension graft is too long. This can be prevented by measuring the distance between the septal caudal edge and the average cruras to calculate the exact size of the graft.
- Deviation of the nasal tip, which results when the graft is deviated or improperly set. It is more frequent when it is set lateral to the septum.
- On rotation and on projection of the nasal tip. This occurs primarily when newly commencing with this technique since one is accustomed to overcorrecting when the columellar strut is used. However, with the septal extension graft the tip does not tend to fall over time and does not require overcorrection.
- Loss of support for the nasal tip. This can appear as an early or late complication and responds to two causes. The first being bad septum fixation technique and the second being a tear in the septal cartilage due to sutures, which occurs more frequently when sharp needles are used
Due to the predictable results offered by this graft, the author uses it in 80% of cases when an increase in projection of more than 2mm is required, when the distance between the middle cruras and the septum is 5mm or more, when the patient has thick skin, retracted columella, when the “tongue in groove” technique is performed, when the septum is short, and when a columellar strut has previously failed.
2. Columellar strut
This graft is the most common in rhinoplasty worldwide and it has a weak and unpredictable support mechanism for three main reasons.
- It is a floating graft, even if it is set to the middle crural or the nasal spine.
- Often, the absorption of cartilage decreases structural support in the long term.
- The force of retractable scars is applied directly to the graft. Due to this it is little used in our practice. Many of our cases are patients who have been re-operated on five years after their first surgery due to the decrease in the projection observed in immediate and early results.
The sole indication for which we use this graft is when we want to strengthen the support mechanisms of the tip or when you want to increase the projection by 2mm or less.
3. Lateral crura strut graft
This type of graft is an invaluable tool in the management of the nasal tip since it offers many advantages.
- An increase in the projection, definition and rotation of the tip. (Images 8-11)

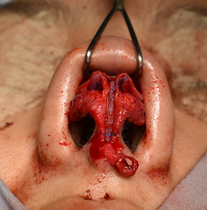
Image 10 (pre, post. Lateral view)


Image 11 (pre, post frontal view)


- It eliminates the bulbosity of the tip. (Images 12-13)
Image 12 (pre, post lateral view)


Image 13 ( pre, post base view)


- It prevents postoperative alar pricking and retraction and provides excellent support to the side wall while retaining the functionality of the nose. (Image 14)
Image 14 (pre, post frontal view)


- It corrects asymmetries and concavities/ convexities of the lateral cruras.
- It is indispensable in repositioning the lateral cruras.
- Reconstructive graft in cases of secondary rhinoplasty with excessive resection of the lateral cruras.
In the management of this graft there are certain complications that the novice surgeon must take note of.
- External valve collapse due to excessive thickness of the graft. This complication can be avoided by using a 1mm thick graft.
- Extrusion or infection of the graft. This can be prevented by a delicate dissection of the lateral crural from the skin of the nasal vestibule, for which a prior hydrodishydrodissectionection is necessary.
- Hard Pollybeak is another complication that happens when the graft is very large so it is recommended to be 4-5mm high, 30mm long, and 1mm wide.
- Extrusion of the suture material toward the nasal vestibule is one of the most frequent complications and it can be avoided by using PDS and knotting the point on the superior side of the lateral rural.
- The repositioning of the lateral crura with this graft is one of the most complex manoeuvres to perform correctly so special attention should be paid to each of the steps when performing it while verifying the symmetry of one side to the other (Image 15).
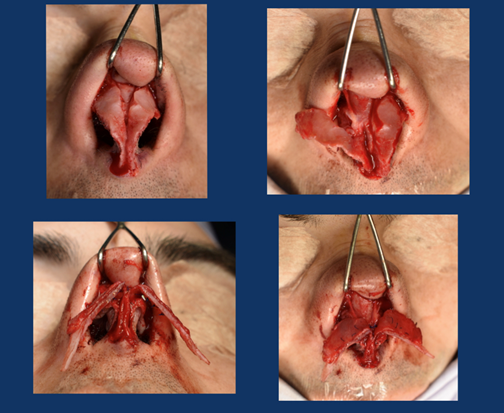
This is why an open surgical approach is recommended and that the lateral pockets, where the strut of the lateral crural is repositioned, are made in the same plane, both starting where the marginal incision ends and directed towards the piriform aperture. Another important manoeuvre when placing the interdomal point is that it should be in an oblique arrangement, where the caudal part is more anterior and the cephalic more posterior. As such, the orientation of the crural changes immediately
4. Alar rim graft
This is a versatile and very useful graft to correct the alar retraction, give extra support to the external valve, improve the contour of the nasal wing, and to prevent or correct the soft triangle retraction. Further, it is relatively easy to place. We prefer to use the articulated type since it is more attached to the structural philosophy in being attached to the dome by way of a graft
A possible complication is that the pocket that is made at the alar edge is very superficial and the graft can be extruded over time.
5. Shield graft
This graft was described by Jack Sheen and popularized by many great surgeons around the world. Personally, we do not consider it to be structural graft, rather, it is a graft that provides definition but not structure or support. It is a graft that should not be used in patients with thin or intermediate skin since it becomes perceivableunder the skin over time and looks unnatural. It is an excellent tool for noses with very thick skin for nasal tip definition and works well for black-skinned population.
The three most frequent complications of this graft are:
- Over projection. This is related to the size of the graft, most specifically with the part of it that protrudes above the domes. It is recommended that it be 3 to 4mm.
- Displacement of the graft is frequent so it is necessary to set it both to the middle crurals and to both domes and to place a graft above the lateral crurals behind the graft in shield, as well as to set it to avoid back displacement (Image 12). It is also important, if it is possible, to place septal extension graft to give stability to the nasal base. (Image 16)

- The other complication is the stigma that is generated over time as the edema disappears and the scar contracture that makes the shape of the graft visible in thin and medium skin. This can be avoided by placing a soft tissue graft, for which we use the perichondrium of costal cartilage or the PAT graft consisting of soft tissue intercrural with the Pitangui ligament.
The use of one or all of the grafts described should be used rationally and with a sound indication so that a natural and functional result can be achieved, as can be noted in the following case. Here, preoperative and one year postoperative images demonstrate the results of a surgery in which a septal extension graft, a lateral crural graft, and a Peck graft were used.














CONCLUSIONS
Structural rhinoplasty was born as a concept when it was described by Calvin Johnson and Dean Toriumi in 1989. Since then it has had a very important evolution based on the principles of conservative tissue resection, structural support, and softened contours. Due to this, the surgeons who perform it have evolved from using the grafts they originally described to using different types of grafts. The philosophy of structural rhinoplasty emphasizes restructuring and remodelling rather than the reduction of the nasal skeleton. The maintenance of structural integrity through grafts facilitates aesthetic results capable of resisting the forces of scar contracture and the results remain stable over time.
It is imperative that all surgeons working with the nose master these techniques. They are essential in achieving long lasting results in various nose types. Like everything in medicine, the most important thing is to make a good diagnosis, in this case, of nasal deformity, to understand the cause of each deformity, and to have a well-designed plan before performing surgery. It is also important to understand that structural rhinoplasty is not applicable to all cases, however, it is increasingly used in our patients. Likewise, good communication with our patients is essential if we are to opt for one of these techniques since there are complications and adverse situations that patients must be aware of.
Disclosures
The authors declared no conflicts of interests or financial interests with respect to the authorship and/or publication of this article.
Bibliography
- Sheen,J.H.,Sheen,A.P.Aestheticrhinoplasty.2ndedition. CV Mosby, St Louis (Mo); 1987
- Tardy,M.E.Rhinoplasty:theartandthescience.WB Saunders Co, Philadelphia; 1996
- Daniel,R.K.Thenasaltip:anatomyandaesthetics.Plast Reconstr Surg1992;89:216–224
- Toriumi,D.M.Structureapproachinrhinoplasty.FacialPlast Surg Clin North Am. 2005;13:93–113
- Gunter,J.P.,Rohrich,R.J.,Friedman,R.M.Classificationand correction of alarcolumellar discrepancies in rhinoplasty. Plast Reconstr Surg. 1996;97:643–648
- Guyuron,B.,DeLuca,L.,Lash,R.Supratipdeformity:a closer look. Plast Reconstr Surg. 2000;105:1140–1151
- Ha, R.Y., Byrd, H.S. Septal extension grafts revisited: 6-year experience in controlling nasal tip projection and shape. Plast Reconstr Surg 2003;112:1929–1935
- Johnson,C.M.J.,Toriumi,D.M.Openstructurerhinoplasty. WB Saunders Co, Philadelphia; 1989
- Johnson,C.M.J.,Godin,M.S.The tension nose:open structure rhinoplasty approach. Plast Reconstr Surg. 1995;95:43–45
- Kridel,R.W.H.,Scott,B.A.,Foda,H.M.T.Thetongue-in- groove techniquein septorhinoplasty: a 10-year experience. Arch Facial Plast Surg. 1999;1:246–256
- Toriumi,D.M.Caudalseptalextensiongraftforcorrectionoftheretr acted columella. Op Tech Otolaryngol Head Neck Surg. 1995;6:311–318
- Toriumi,D.M.Structureconceptinnasaltipsurgery.OpTechPlast Reconstr Surg. 2000;7:175–186
- Toriumi,D.M.Rhinoplasty:facialplasticsurgery:theessentialguid e. Thieme Medical Publishers Inc., Stuttgart, Germany; 2005 (223–53)
- Gunter,J.P.,Friedman,R.M.Lateralcruralstrutgraft:techniquean d clinical applications in rhinoplasty. Plast Reconstr Surg. 1997;99:943–955
- Rohrich,R.J.,Raniere,J.Jr.,Ha,R.Y.Thealarcontourgraft:correcti onand prevention of alar rim deformities in rhinoplasty. Plast Reconstr Surg.2002;109:2495–2505
- Kim,D.W.,Toriumi,D.M.Nasalanalysisforsecondaryrhinoplasty.F acial Plast Surg Clin North Am. 2003;11:399–419
- Whitaker EGJohnson CM Jr Skin and subcutaneous tissue in rhinoplasty. Aesth Plast Surg. 2002;26119
- Anderson JRJohnson CM JrAdamson P Open rhinoplasty: an assessment. Otolaryngol Head Neck Surg. 1982;90272- 274
- Johnson CM JrToriumi DM Open structure rhinoplasty: featured technical points and long-term follow-up. Facial Plast Surg Clin North Am. 1993;11- 22