Rhinoplasty surgical procedure is one of the most interesting and complex aesthetic surgical procedure… proved by the number of secondary rhinoplasties.
The main goal of aesthetic and artistic rhinoplasty is to achieve a natural look of beauty enhancement and most harmonious face.
There is no one standart rhinoplasty but many rhinoplasties that have to suit to each patient.
Quest of beauty is everyone demand for a better well being and self confidence.
Rhinoplasty has to improve facial aesthetics and to improve nasal breathing function which is also an important point for patients.
Nasal tip is a key point of facial harmony. It is mobile and its mobility depends on muscle activity of the nasal spine area and nostril area. The nasal position is of great importance for an harmonious facial balance. The shape and position of the nasal tip are defined by static and dynamic anatomical structures, that the facial plastic surgeon has to understand for a precise correction and a successful outcome. The skin and its thickness also plays a role in the global shape of the tip and its contours. Nasal tip must be analysed as a part of the nose and as an individual anatomical strucutre.
The base of the nose is analysed at the same time as it holds the tip in a position and is part of the mobile nose.
Nasal tips are defined by their projections, rotation and contour definition.
Surgical anatomy and nasal tip projection and rotation
| The base of the nose is made of cartilages, variable in shape and resistance. Covering tissues as skin are very different from a patient to another in their elasticity and thickness. The projection and position of the nasal tip depends on the shape of tip cartilages, their supports (nasal septum), the tip muscle activity (mainly muscle depressor septi) and the type of skin. | 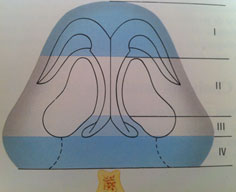 |
| On an inferior view, 4 segments should be defined in the nasal base. |
I) The Apical segment, is the lobule of the nasal tip where intermediate cruras and domes are.
There is divergence angle that yield to a distance in between alar domes. Increase of this segment can be performed by a modeling tip procedure or dome section (Goldman).
| Use of cartilage grafts can help to lenghten this segment and increase the projection. These grafts modify both projection and nasal tip contour | 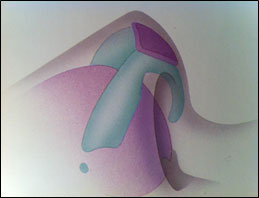 |
II) The collumellar segment
Columella plays a major role in an aesthetic approach. It is located between the apex of nostrils and the bottom part of the columella where it becomes wider. No lenghtening is possible at this place as skin and cartilage are very adherent.
III) Mesial cruras segment
This segment is defined by a divergence between both mesial cruras. Lenghtening of this segment can be achieve by soft tissue excision (between mesial cruras) and both cruras transfixing sutures. This yield to a light gain of projection and light nasolabial angle opening.
IV) « supra-nasal spine » segment
This segment is located between the nasal spine and the lower part of mesial cruras. This segment is cartilage free and is extensible, by using columellar struts that are supported on the nasal spine.
Nasal tip contours
The ideal nasal tip should have specific characteristics, which are not always gathered :
- Nasal tip autonomisation ,when its projection is lightly longer than the dorsum one.
- Visualisation of cartilage shapes and relief, in cases with thin skin.
- “lobulo-columellar double break” that individualizes the apical lobule segment and the columella.
Simplified artistic approach of nasal tip projection, using Goode’s methodology
Goode’s method is based on a trigonometrical analysis of the nose and its dimensions. On a profile view, the fist line is traced from the nasion (anf) to the lateral nostril alar groove (af) . The second line is perpendicular to the first one, crossing the tip of the nose (p).
| Distance from (af-p) should be approximately 55 to 60% of the distance (anf-p). |  | ||
| Distance from (af-p) should be approximately 55 to 60% of the distance (anf-p). | ||||
|
A simplified method, originating from the previous one, gives quick information on tip projection : A tip projection is right when 50 to 60% of the line (anf-p) is forward a vertical line crossing the upper lip on a profile view.
| Tip projection and rotation : linked and dissociable! |  | ||
| Tip projection and rotation : linked and dissociable! | ||||
|
Relations between tip projection and rotation
Relations between tip projection and rotation implies visual illusion.
- The dorsum shape, mainly in cases of convexity, gives a visual illusion of drooping tip, eventhough the nasolabial angle remains open!
- Conversely for a concave dorsum where a visual illusion of excessive tip rotation occurs (“jumping nose”).
- The concept of tip autonomisation helps to limitate this visual illusion, as the supra tip depression separates both structures : dorsum and tip.
- Upward tip rotation give a visual illusion of nose lenghtening.
Analysis of relations between nasal tip projection and rotation has been defined by Anderson with the “tripod concept“.
Tripod Theory and concept.
The tripod concept of tip projection, support, and rotation described by Anderson provides an understanding of the dynamics of tip rhinoplasty. The anatomy of the two alar cartilages forms a functional tripod that provides tip support. The right and left lateral crura comprise two legs of the tripod, and two conjoined medial crura function as the third leg. Anatomically, the medial crura are shorter than the lateral crura. The medial crural foundation is supported by the attachments to the superior and inferior septum. (Punjabi 2008)
Tip Rotation
The tripod concept of nasal tip support and the major and minor tip support mechanisms must be considered in nasal tip rotation especially ptosis. In addition, the integrity of the medial and lateral crura, the attachment of the medial crural feet to the caudal end of the quadrangular cartilage, and the scroll-like attachment of the caudal end of the upper lateral cartilage to the cephalic margins of the lateral crura are the major tip support structures to consider. The minor tip support mechanisms include:
- The dorsal cartilaginous septum,
- The interdomal ligaments,
- The nasal spine,
- The membranous septum,
- The alar attachments to the skin.
Alterations in the size, shape, and integrity of the limbs of the tripod, together with the disruption of the major and minor tip support mechanisms, result in profound alteration in tip rotation.
A major step in any tip rotation procedure is the cephalic resection of a portion of the lower lateral cartilage. Such a resection leaves a gap between the lower lateral and upper cartilages. This gap is partially closed as the lower lateral cartilages scar upwards, resulting in tip rotation. Two basic types of cephalic cartilage resection include those techniques that preserve an intact strip of cartilage, and those that interrupt the entire lower lateral cartilage. Complete strip techniques resect a variable amount of the cephalic lower lateral cartilages. More cartilage is resected for a greater amount of volume reduction and for a greater degree of cephalic tip rotation. The complete strip can be weakened in several ways to assist in cephalic rotation. These methods must, however leave the lower lateral cartilages with sufficient strength to maintain tip support. For patients who have significant tip depression, interrupted cartilage techniques may be required to achieve sufficient tip rotation. The interruption of the lower lateral cartilage releases the spring-like tension on the nasal tip and allows much greater cephalic rotation of the tip. However, interruption also destroys a major tip support mechanism and also leaves the nasal tip subject to less predictable scar formation and asymmetries.
Adjunctive tip rotation maneuvers are often necessary to achieve adequate tip rotation, especially when complete strip techniques are used, as discussed above. Various degrees of excision of the caudal septum can effect tip rotation. This is because excision of the caudal septum can provide room for the infratip lobule to ascend during healing. The medial crura should be left attached to the caudal septum when possible, though, or resutured if the attachment is violated. Excessive caudal septum resection should be avoided, as this can lead to loss of cephalic tip rotation and projection. A high transfixion incision can be used on the caudal septum with excision of a triangular wedge of septal cartilage. This allows immediate cephalic tip rotation, though projection may be sacrificed if resection is excessive. Excision of redundant portions of the upper lateral cartilages may be necessary if the alar cartilages are altered to a degree that they impinge on the upper lateral cartilages. This resection should be conservative to reduce the likelihood of resultant depressions in those areas. Excision of excess vestibular skin can create a minor force for cephalic rotation. Division of the depressor septi nasi muscle decreases dynamic tip depression and can greatly complement other modalities of tip rotation. Imbrication of this muscle has been shown to have greater and longer-lasting effect than simple division. Proper taping of the nose after nasal surgery may provide tip support during the healing process.
Other tip rotation techniques can create the appearance of tip rotation by altering the nasolabial angle. Morselized cartilage grafts into the columella-philtrum junction can result in increasing the nasolabial angle so that the illusion of tip rotation is created. Cephalic resection of the lower lateral cartilages to a point beyond the tip defining points can lead to a supratip dip that creates the illusion of tip rotation.
Tip Projection
After primary rhinoplasty there is a postoperative decrease in nasal tip projection unless steps are taken to increase the length and strength of the medial crural segment. Either the cartilage-delivery or cartilage-splitting approach weakens or disrupts the support mechanism of the nasal tip. One of the ways to preserve tip projection after nasal surgery is to resuture the medial crural footplates to the caudal septum when they are detached. Additionally, a caudal strut may be fashioned from autogenous cartilage. The caudal strut should be fashioned with a curve that matches the collumella and should be positioned and sutured between the medial crura. A pocket is dissected between the medial crura and the graft is placed here. The graft should not project beyond the domes of the lower lateral cartilages in order to avoid a tented up appearance of the nasal skin. The graft should not rest on the nasal spine, as displacement from the spine will cause the patient to experience nasal clicking and discomfort. Often the caudal strut can be sutured to the caudal septum.
Medialization of the lateral crura of the lower lateral cartilages can enhance tip projection. This can be accomplished in several ways. One method that is rarely used is the division of the lateral domes of the lower lateral cartilages and suturing of these cartilages together over the midline with permanent sutures. Although this procedure increases tip projection, it may also lead to a tent-pole appearance of the nasal tip. Another procedure, often referred to as the “Lateral Crural Steal”, involves rotation of the lateral crura medially and placing an interdomal stitch to hold the crura in place. This procedure narrows the nasal tip, increases tip projection moderately, and leads to mild cephalic tip rotation.
Tip grafts can achieve the effect of increased nasal tip projection. The tip grafts can be of varying sizes and shapes. The grafts are placed in positions that enhance bilateral tip-defining points and therefore achieve maximum aesthetic results. Stabilization of the graft must be assured with sutures or creation of a snug pocket so that the graft does not become displaced. A single graft that is trapezoid or shield shaped can be fashioned and placed in the midline to overlap both tip defining points. Some surgeons, however, utilize rectangular or circular smaller grafts and suture them individually over each dome so as to more closely approximate the natural separation of the tip defining points.
Other methods can create the illusion of increased tip projection. One such method is the removal of a dorsal hump, which makes the nasal tip appear more prominent. Cephalic rotation itself can create the illusion of tip rotation.
Reduction of tip projection is occasionally required. Reduction of tip projection is best achieved by assessing the cause of the problem and sacrificing major and minor tip support mechanisms directly related to this. Often this overprojection is due to an overdeveloped quadrangular cartilage of the septum. In such patients, the septal cartilage may place tension on the lower lateral cartilages, leading to overprojection. This can be corrected by reduction of the dorsal septum. When the lower lateral cartilages are responsible for overprojection, an interrupted strip technique with conservative resection of a rectangular wedge of cartilage with resuturing will aid in correcting the problem. An alternative method is the lateral crural overlay technique discussed above. Another tip support mechanism can be sacrificed to reduce tip projection via the transfixion incision, which sacrifices the medial crural footplate’s attachment to the caudal septum. Most of the reduction of tip projection methods discussed above will lead to widening of the nasal ala. Wedge excision of the alar bases may be necessary to achieve nasal harmony.
Tip Definition
One of the most common problems encounter when addressing tip definition is the bulbous tip. In order to correct this deformity it is important to recognize the underlying problem. The most common causes of bulbous tip are the wide interdomal distance, widening of the domes, weak lower lateral cartilage and thick skin with lack of definition. Many of the already describe maneuvers address the definition. The transdomal suture in particular plays an important role in definition by narrowing the domal structure and by end result the tip. Interdomal suture and medial crura suture will also improve definition by decreasing the interdomal distance. The dome division with binding suture significantly increase tip definition by decreasing the domal width.
Medical rhinoplasty and nasal tip
Medical rhinoplasty is a minimal invasive procedure, temporary with impressive outcomes.
The use of dermal fillers and botulinum toxin permits to modify the shape and position of the nasal tip, by performing a nasla sculpture. Fillers are hyaluronoic acid ones and muscle blockage are performed wioth botulinum toxin A.
Clinical cases
-Exemple of hypoprojected tip
-Overproject nose
-Download tip attraction by depressor septi nasi musclel action
Clinic case n°1
Overproject and falling tip. Secondary rhinoplasty.
Section of nasal septum. Sheen graft and mésiales sutures.
|  |  |  |  | Before | After | ||||||
| | |||||||||||
| | |||||||||||
| Before | After |
Clinical case N° 2
Medical Rhinoplasty
Hyaluronic acid injection ( Tip, Hump and collumella)
Botulinum Toxin injection : Depressor septi nasi muscl, Dilator muscle and common elevator muscle.
| Before |  |  |  | After |  |  |  | ||||||||||||||||
| Before | ||||||||||||||||||||||||
| | | ||||||||||||||||||||||
| After | ||||||||||||||||||||||||
| | |
References
– Anderson J.R., Ries W.R. Rhinoplasty: emphasizing the external approach.
The American Academy of Facial Plastic and Reconstructive Surgery,
Thieme Inc., New York, 1986.
– AIACH Gilbert. Atlas de rhinoplastie. Masson éditions Paris. 1996.
– REDAELLI Alessio, BRACCINI Frederic. Medical Rhinoplasty. Basic principles and clinical practice. Ed. OEO Firenze 2010.
– BRACCINI F, DOHAN EHRENFEST DM. Medical rhinoplasty: rationale for atraumatic nasal modelling using botulinum toxin and fillers. Rev. Laryngol. Otol. Rhinol (2008; 129(4-5):233-8.
– BRACCINI F, PORTA P, THOMASSIN JM.
Mini-rhinoplasty. Rev Laryngol Otol Rhinol.
2006; 127,1:15-20.
– PARIS J, FACON F, THOMASSIN JM. Saddle nose surgery: long term aesthetic outcomes of support grafts. . Rev Laryngol Otol Rhinol. 2006; 127(1-2):37-40.