ABSTRACT
The “structure rhinoplasty” avoids the typical unfavorable outcomes resulting from old fashion “resective techniques”. Reconstructing the nose with support tip grafts helps us to be more accurate in projection, rotation and definition.
In 2009 we started to use septal extension graft (SEG), which was the milestone to get more predictable long term tip projection and rotation results. But its design depends on a strong and aligned septal cartilage. Otherwise tip asymmetries could be increased. Septal caudal replacement graft (SCRG) was the key to find the solution in cases that L-Strut was not reliable. Then, we could find a new approach to the majority of the asymmetries.
We also show how to use the “extended pedestal spreader grafts” (EPSG) that will allow us not only to hold the tip graft but also to create a more functional and aesthetically attractive middle vault.
Finally, we are going to focus on how to solve the most frequent situations of lack or excess of tip projection and the methods to control the definition of the tip and prevent from “unitip deformity”.
Key words: nasal tip, septal extension graft, caudal septal replacement graft, extended pedestal spreader grafts, tip support, caudal septal reconstruction.
INTRODUCTION
In Rhinoplasty, to achieve long term and stable results it is important to give support to the nasal tip. For this purpose, we need to use cartilage grafts. This is the basis of the “structure rhinoplasty” concept. This technique avoids the typical unfavorable outcomes resulting from old fashion “resective techniques”. Support tip grafts help us to be more accurate in projection, rotation and definition. Nowadays the most important challenge is to get as much symmetry as possible in the “structure rhinoplasty”.
In 2000, we started placing free strut grafts between media crura of the LLC to strengthen the tip in order to prevent from future deprojecting and drooping that resulted from healing contraction that happened as time passed. Nevertheless, in some cases, especially those related with heavy skin sleeve would lose the result we obtained at immediate postop. This is the reason why in 2009 we started to use septal extension graft (SEG), which was the milestone to get more predictable long term tip projection and rotation results. With the SEG we manage to solve the projection and rotation challenge, but its design depends on a strong and aligned septal cartilage. Otherwise tip asymmetries might be increased. Septal caudal replacement graft (SCRG) was the key to find the solution in cases where the L-Strut was not reliable. Then, we were able to find a new approach to the majority of the asymmetries.
In short, we have nowadays two main methods to hold the tip in the correct position: SEG and SCRG. In this Chapter we will discuss the appropriate technique to be used in each case. We will also show how to use the “extended pedestal spreader grafts” (EPSG) that will allow us not only to hold the tip graft, but also to create a more functional and aesthetically attractive middle vault.
Finally, we are going to focus on the design of a favourable tip contour, how to solve the most frequent situations of lack or excess of tip projection and the methods to control the definition of the tip and prevent from “unitip deformity”.
DECISION MAKING
First, we need to decide whether we are going to use SEG or SCRG. Right after we finish the open approach and dissect both mucoperichondrial flaps, freeing the septal cartilage from any attachments, we can assess the true shape of the septal cartilage (watch video 1 “dissection, hump resection and osteotomies”). At this moment we have to evaluate the following four conditions: 1) to be in the midline, 2) to be properly attached to the nasal spine, 3) not to be deviated (c-shape, italic or S-shape), 4) not to be too weak or thin to support the structure (Figure 1).

Pearls: The decision should be made previous to the chondrotomy, because for the SCRG technique, we need as much cartilage as possible, and If we get the L-strut and then we decide to go for the SCRG, we will miss 10 essential mm for the graft.
Extended Pedestal Spreader Grafts
Before moving on with SEG and CSRG techniques, we will focus on the extended pedestal spreader grafts1. Because they are a milestone in the making of the structure.
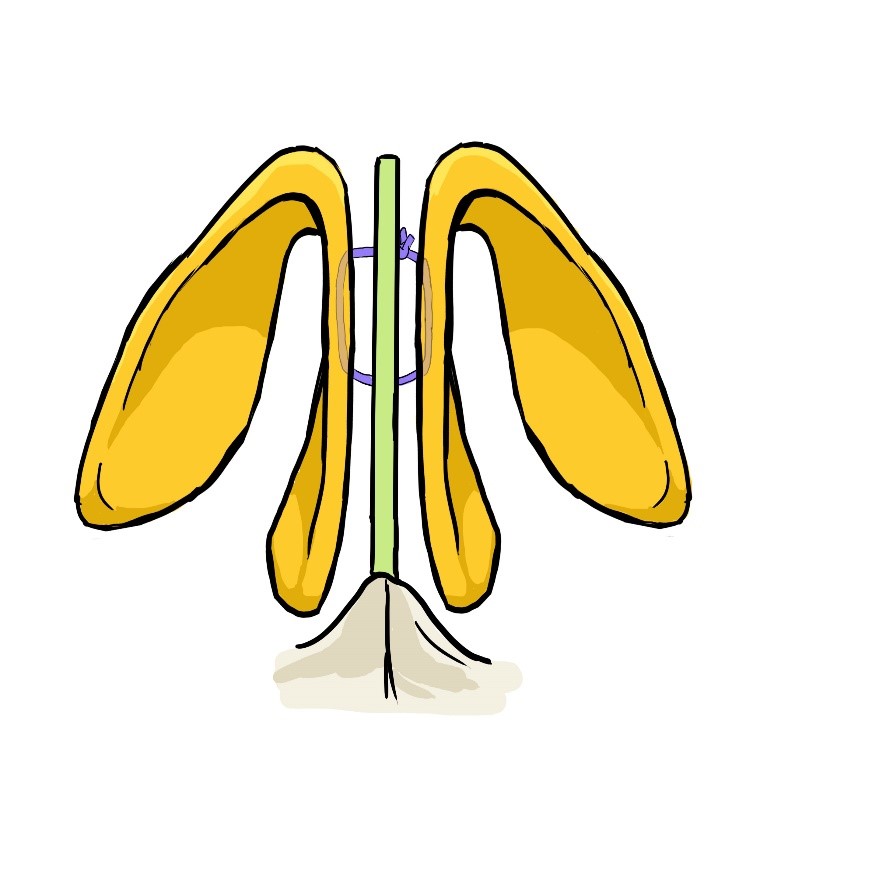
Why “Extended”: Because the caudal end of the spreader graft extends beyond the line of caudal septum.
Why “Pedestal”: Because we place the spreader grafts 2 mm below the line of dorsal septum in order to use it as the basis (pedestal) for the ULC mount. This will restore the normal dorsal width. With this maneuver we also give tension to the nasal lateral wall to get a functional valve result (Figure 2).
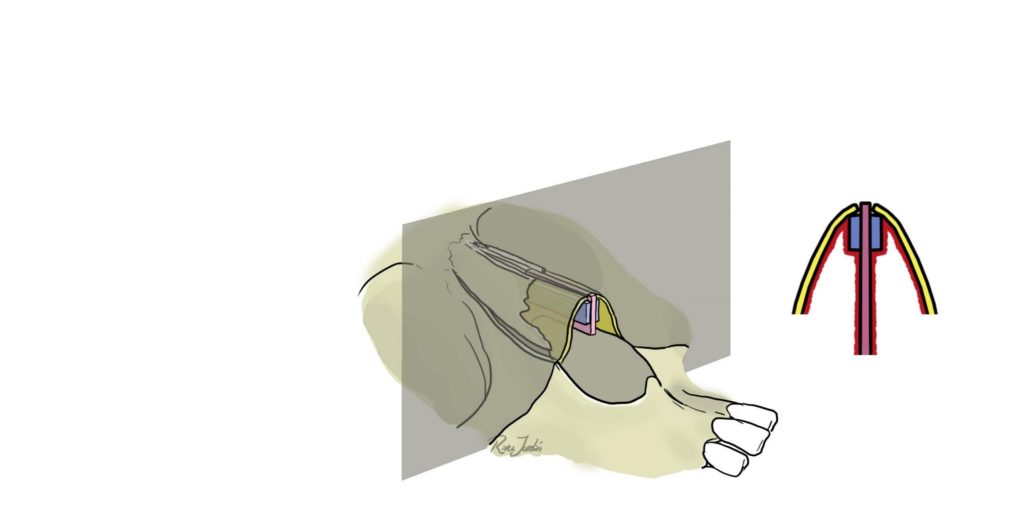
Pearl: 1) It is advisable to look for the longest parts of the harvested cartilage for the EPSG making 2) EPSG should be narrowed in the caudal end to avoid visibility bumps on both sides of the columella, and also because it could eventually block the airway.
Thoughts: Even though after many years we have used the spreader flaps instead of the spreader grafts, we have noticed that in many cases the dorsa could bend after the healing process leading to a deviated nose. The main reason for that is that a weakened L-strut following chondrotomy may not be strong enough to keep the dorsum straight. This bending situation is pictured specially with facial expressions. Then, we concluded that extended spreader grafts are necessary to have a reinforced architecture in the remaining septal dorsum.
Septal extension Grafts (SEG) (Video 2: Septal Extension Graft)
If the septal cartilage does not have any of the above mentioned deformities (Figure 1), we will use this technique. This is about placing a graft that extends septal cartilage caudally and anteriorly to get the tip at the desired position.
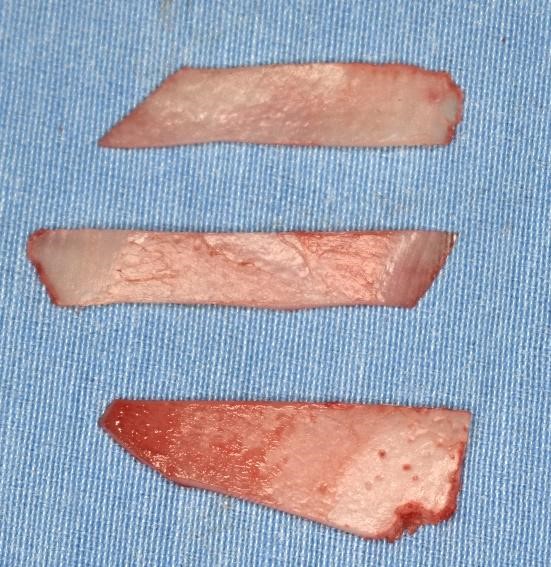
With the harvested septal cartilage, we need to design three grafts. Two spreader grafts (25 x 5 x 1mm) and one septal extension graft (25 x 7 x 1mm in the upper part and 25 x 2 x 1 in the lower part) (Figure 3).
Tricks in septal extension graft
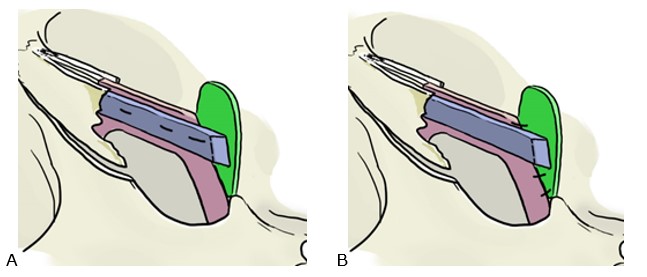
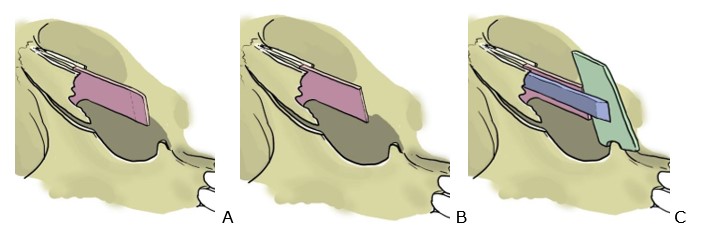
- Spreader grafts are mounted in the first place in order to make much easier the suture of the septal extension graft (Fig. 4).
- Septal extension graft should to be placed as an end-to-d attachment to prevent asymmetries of the tip and columella (Fig. 4).
- It is advisable to straighten the original convexity shape of the caudal septum border with an 11 blade to match exactly the septal extension graft (Fig. 5).


Septal Caudal Replacement Graft (Video 3: SCRG)
If for any of the mentioned reasons (septum not in midline, weak septum, bending septum), we cannot trust in caudal septum to hold the septal extension graft, we proceed with septal caudal replacement graft.
In this situation we harvest the septal cartilage including the caudal margin and we leave only a 7-15 mm strip in the dorsum line. From this cartilage we design three grafts. Two for the EPSG and one for the SCRG.
The SCRG is fixed to the nasal spine posteriously and to the EPSG anteriorly. First, we suture the EPSG to anterior nasal spine with a cross suture (Fig. 7).
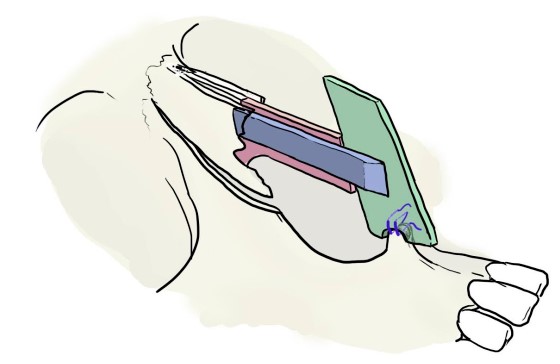
It’s important to leave the periostal tissue on the anterior nasal spine for two reasons: first, to avoid the need of making a small hole in the nasal spine for the suture; and second, to have a soft tissue absorbing and avoiding the direct contact between the cartilage and the bone.
With a rongeur we make a notch in the inferior part of the graft to be in contact with the anterior nasal spine; thus, it prevents the anteroposterior graft movement (Fig. 7, 8 and 9).
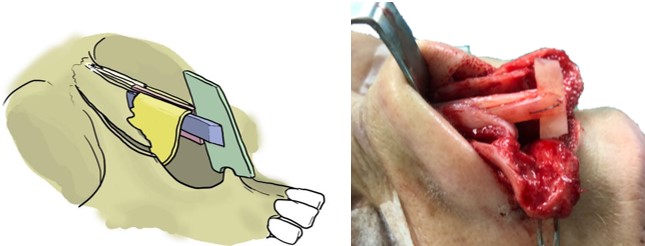

The notch should not exceed 2-3 mm from the caudal border of the graft to prevent an undesirable lowering of the columella and a horizontal crease of the upper lip.
Pearl: we strongly recommend to use the thickest part of the septal cartilage harvested (which is the part originally joint to the perpendicular ethmoid bone) as the basis to be attached to the spine. Thick could be up to 3mm.
It is easier to place first the CSRG to the spine and then the spreader graft. Otherwise the remaining septal strip could be at risk with manipulation.
We always link the CSRG and the remaining septal strip into an end-to-end attachment. To avoid the tip down rotation, we will need to resect at least 3mm of the remaining septal strip caudally (Fig. 10)

Final steps of the tip structure (Video 4: Tip definition and i-TEGs)
To continue with the design of the tip structure, first, we need to define the subnasale point. For this purpose, we will make a suture that includes both footplates and the tip supporting graft. Thus, preventing from hanging columella and columella retraction. Another “U” suture is placed for medial crura fixation (Fig. 11)
Then we check if the domes reach desired tip projection with the required tension of the lateral crura. If so, then we suture the domes to the tip supporting graft. The suture must be placed on the cephalic part of the domes to guarantee the diamond polygonal shape2. This situation generally happens in 90% of the cases. The remaining 10% is as follows:
- We need more projection: in this case we can use an onlay “Peck” graft3, as many layers as required. Cephalic trimming would be the perfect graft for this case.
- After we suture domes, we notice an over projection of the tip. In this case we cannot deproject the tip by just placing the domes posteriorly, because it will create a “relaxed” tension in the lateral crura4 that can generate a valve insufficiency due to the recurvature of the lower lateral cartilage. To prevent the loss of tension, we do a modified “Lipsett Maneuver”5, which consists in resecting a portion of middle crura and creating new domes laterally by the “lateral crura steal” maneuver.
I-TEG
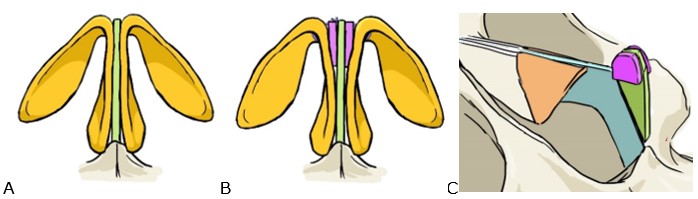
Once we suture the domes to the tip supporting graft, we may notice that the tip shape is very narrow. If not corrected, we will end up with a “unitip deformity”. This specifically applies to thin skin on over-defined domes. Our aesthetic concept is always to create a polygonal shape of the tip, following Baris Cakir’s ideas2. To achieve the desired polygonal shape, we design a specific graft called “i-TEG”: Interdomal Tip Expanding Graft consisting of two pieces of 5mm x 5mm cartilage that we place laterally on both sides of the tip supporting graft (Fig. 12). We have been using this novel graft for the last 3 years in 25% of the cases.
Conclusions
To achieve predictable, long-term and symmetrical results, we need to support the structure with an aligned, strong and reliable graft. Both SEG and CSRG are two powerful tools to achieve this purpose. During the last year we decided to use the CSRG rather than the SEG because we consider CSRG to be a more reliable structure to hold the tip. Our rate is 80% for the CSRG and 20% for the SEG, in the last year. Our question is: Will the CSRG be the next Gold Standard to hold the tip?
Bibliography
- Milos Kovacevic, Frank Riedel, Abdülkadir Göksel, et al. Options for Middle Vault and Dorsum Restoration after Hump Removal in Primary Rhinoplasty; Facial Plast Surg 2016;32:374–383.
- Baris Cakir; Surface Aesthetics in Tip Rhinoplasty: A Step-by-Step Guide, esthetic Surgery Journal; 2014, Vol. 34(6) 941–955.
- Peck GC. The onlay graft for nasal tip projection. Plastic Reconstruction Surg. 1983; 71:27–39.
- Richard E. Davis, MD. Lateral crural tensioning for refinement of the wide and underprojected Nasal. Tip: Rethinking the Lateral Crural Steal, Facial Plast Surg Clin N Am 23 (2015) 23–53.
- Lipsett EM. A new approach surgery of the lower cartilaginous vault. AMA Arch Otolaryngol 1959;7042- 47.
- Hossam M.T. Foda, MD; The Caudal Septum Replacement Graft; ARCH FACIAL PLAST SURG/VOL 10 (NO. 3), MAY/JUNE 2008.
- Dean M. Toriumi, MD1; Subtotal Septal Reconstruction: An Update; Facial Plast Surg 2013;29:492–501
- Byrd HS, Andochick S, Copit S, et al. Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg. 1997;100:999–1010