Introduction:
Rhinoplasty is one of the most difficult procedures in the field of facial plastic. There is significant number of patients end up with poor outcomes. Many of these poor outcomes could be avoided by good surgical judgment and decision making.
To achieve a very efficient dorsal hump, a proficiency of skills and technique, an in-depth understanding of anatomy and aesthetic ideals, usually surgical manoeuvres and technique selection depend on carefully patient preoperative analysis to anticipation and prevention of complications. At the end of the operation, an elegant dorsal profile with aesthetic lines that provide balance and harmony to the face without compromising the nasal functions.
from the anatomical point of view the nasal bones overlap the upper lateral cartilages (ULCs) which is a part or fused to the cartilaginous nasal septum, creating the M-shaped of McDonald’s, at the same time The septum solidly articulates with the perpendicular plate of the ethmoid forming a very important landmark in the surgery of Rhinoplasty “RHINON”.
Unfortunately, hump removal destroys this elegant natural anatomy of the middle and upper third of the nose, so the most important surgical step is to rebuild the middle vault immediately, to avoid nasal dorsal collapsed, irregularities’, airway obstruction (internal nasal valve) &open roof deformity.
Ideally, nasal dorsum lies about 1-2mm posterior to a line drawn from the nasion to nasal tip. In women, the dorsum should be straight to slightly concave with a slight supra tip break while in men, it should be straight to slightly convex.
Aesthetic facial proportions according the angles, should be carefully evaluated, and the ideal nasal proportions 3-4-5 should be also considered as under-projected tip may create the illusion of a dorsal hump & A deep radix can give illusion of a short nose with a dorsal hump.
Hump Removal:
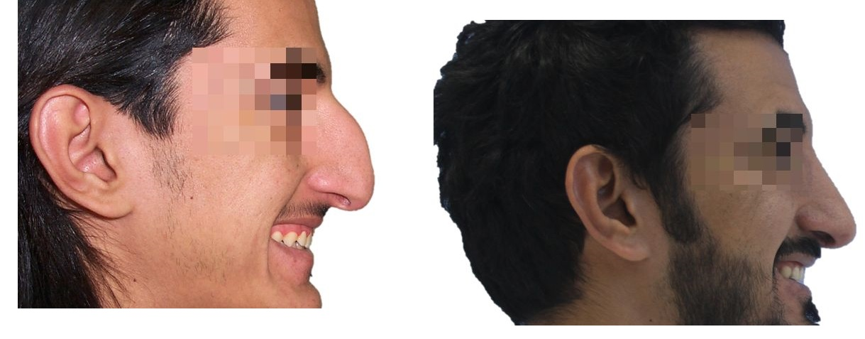
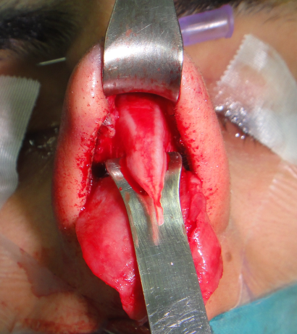
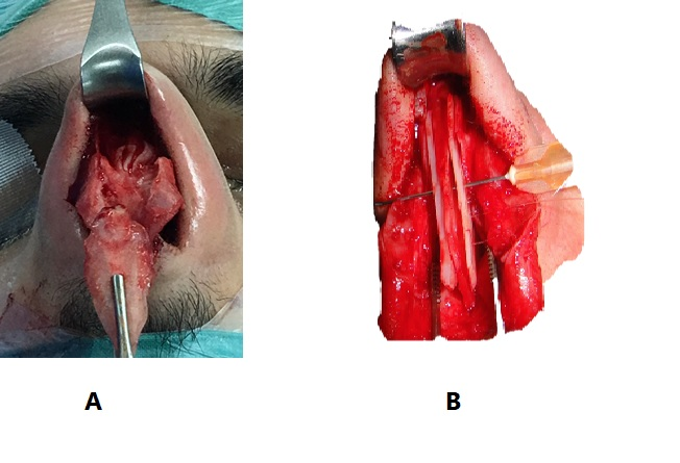
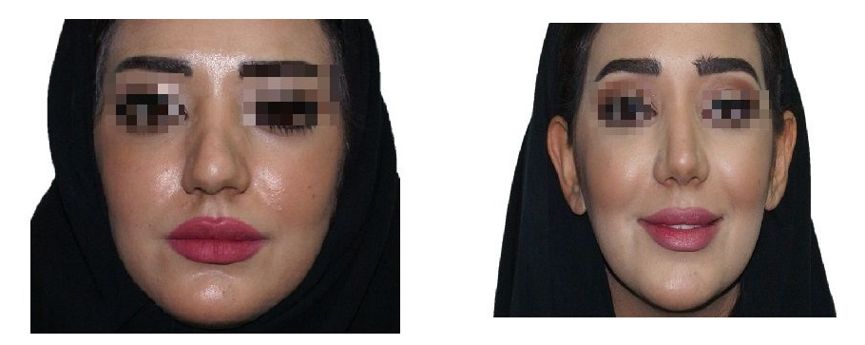
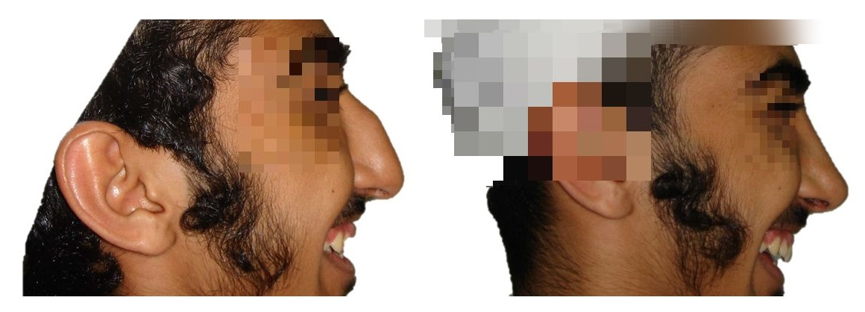
Surgical Resection of hump is a common step in rhinoplasty involves the radix relationship and intrinsically height and base width of the Osseo-cartilaginous vault. There are several ways of excising the dorsal hump, the cartilaginous hump can be resected with a scalpel or scissors while resection of the boney hump requires an osteotome, a saw, or a rasp. (1) (Figure 1&2 )
The external approach is applied for most cases, which offers several advantages such as:
- Direct visualization of the tip cartilages in their natural, undistorted anatomical position.
- Adequate diagnosis of the existing deformity.
- Exact placement of grafts and implants.



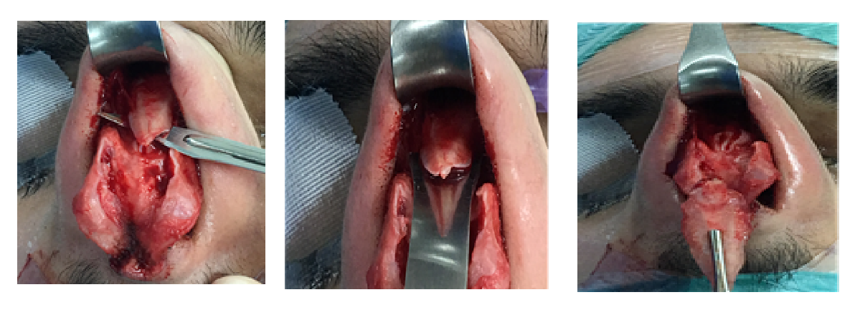
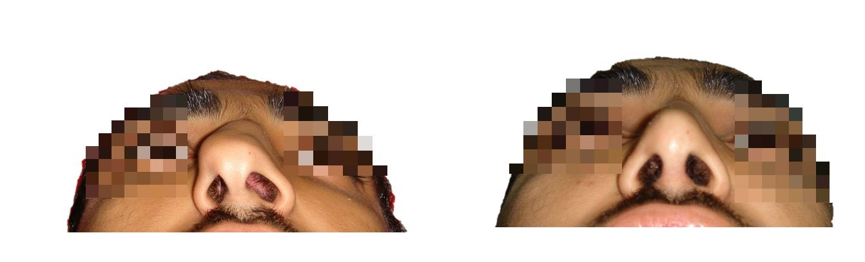
rasping is a good conservative option that allow a gradual hump reduction rather possible, to avoid over-resection & ensure that adequate hump resection has been achieved. (Figure 3)
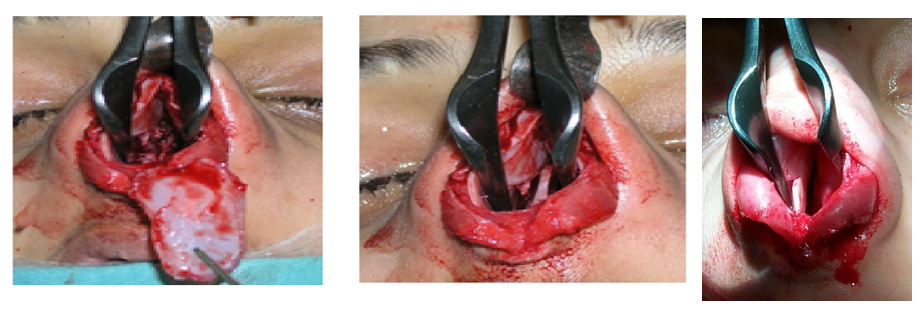
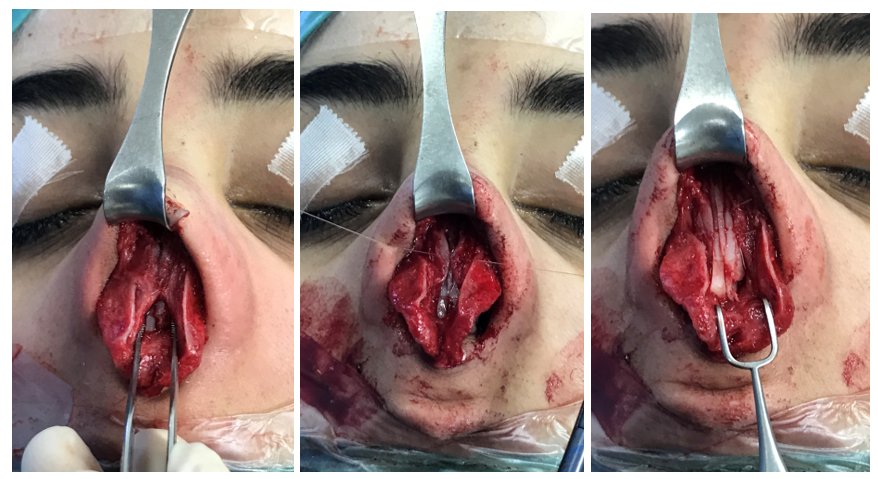
In our hand Dorsal hump resection is usually done in an incremental fashion, starting by piercing the cartilaginous hump with scalpel 11, then sweep it inferiorly toward the anterior septal angle, then we apply a very sharp osteotomy for the bony vault. after removal of the hump we use the rasping to smoothen the bony edges. (Figure 4),
In septoplasty we should preserve at least 10 -12 mm of the dorsal and the caudal septal cartilage that will maintain and support the nasal middle third to prevent saddle deformity. (Figure 5)

Pseudo-hump:
In low radix, someone can preserve a dorsal fullness by augment the nasofrontal angle and then lower the dorsum if needed. If surgeon attempt to resect the pseudo-hump, patient will end up with over-resection. (Figure 6)
Camel Back Hump:
On the other hand, a deformity such as camel back hump is corrected by dorsal onlay grafts. When there is a depression above and below a mid-dorsal hump (camel back hump) then rasping the hump can result in saddle nose deformity. In these cases, a graft should be placed above and below the mid-dorsal hump. (Figure 7)
Open Roof Deformity:
“open roof” deformity is one of the common results after hump removal without rebuilding the middle vault. (Figure 8) Spreader graft or flap with or without a dorsal only graft are required before performing the osteotomies in order to prevent collapsing of the nasal dorsum and avoiding such deformity. Spreader grafts are essential to avoid functional impairment and Middle vault nasal deformity (inverted-V). (Figure 9)


So, the major step following hump removal in rhinoplasty is rebuilding the middle vault. To do this, spreader grafts is the major tool for most surgeons. the spreader flaps have started to be used as well if possible, with or without the spreader graft.
Instead of trimming the ULC to match the newly established dorsal profile, the excess vertical height dissected away from the septal cartilage and issued to create bilateral inwardly folded cartilage flaps that are sutured to the upper margin of the dorsal septum to stabilize the middle vault. (2)
The methods in preserving and reconstructing these vital anatomical middle vault structures can be broadly done by one of these categories:
- the spreader graft technique (Figure 10)
- the spreader flap technique
- Or using both techniques together
the spreader graft method involves donor cartilage, while the spreader flap method makes use of the excess height of the medial portion of the upper lateral cartilages in patients that possess a cartilaginous hump. Both the preserved upper lateral cartilage and the donor cartilage are located along both sides of the dorsal septum in order to prevent a valve collapse (functional impairment) and to provide a harmonious and natural looking contour (3)

The dorsal hump varies differently among patients, especially among our patients, in which the most reductions are cartilaginous humps, which makes spreader grafts essential for any patients to avoid possible function impairment or deformity in the middle nasal vault. (Figure 11 )
Reasons to use spreader flaps or spreader grafts: (4)
- Reconstitute the anatomy of the middle vault.
- Avoid middle vault collapse.
- Restore or maintain the internal valves
- Recreate the brow-tip aesthetic lines
- Splint deviated dorsal segment of the nasal septum
- Re-Create a smooth transition at the key area

Prevention of Possible Complications:
The aesthetic natural anatomy of the middle and upper third of the nose is spoilt during the hump removal procedure. This middle third consists of the ULC (upper lateral cartilages) and the lower third of the nasal bone. There is a unique transition between these structures and the underlying septal cartilage and ethmoid bone. When hump removal is done, there is a disturbance of the relation between these structures. this may cause problems (aesthetic as well as functional) such as internal nasal valve collapse and the inverted V deformity.
- Internal Valve Collapse:
- Inverted V deformity:
The middle third is as important for cosmetic reasons as it is for functional reasons. Deviations, inverted-V deformities and collapsed upper lateral cartilages are possible sequalae with patients that have small nose bones, fragile upper lateral cartilages, or deviated septum. Narrow middle third of the nose can happen if hump removal was done without inserting spreader grafts in some cases.
Deformities as a result of a collapsed internal nasal valve often causes nasal obstruction. During the reduction of the dorsal hump, the horizontal portion of the middle nasal vault is resected at the junction of the nasal septum and the upper lateral cartilages. Patients that have weak upper lateral cartilages can show a noticeable collapse years after the surgery. The best way to correct the deformity and restore nasal valve functions is by using spreader grafts. (Figure 12)
This condition is especially prevalent in patients that have “tension nose deformity”. Patients that have fragile upper lateral cartilages and thin nasal skin also tend to have a distorted middle nasal vault after the reduction of the dorsal hump.
This surgical removal of the upper lateral cartilages from the dorsal septum often causes malposition, pinching, and concave collapse of the upper lateral cartilages.(4)
- In crooked nose both functional and aesthetic problems must be addressed. This is very important especially when associated with hump resection. Since the nasal bones are are unequal in deviated noses together with the deviated septum, more bone should be resected on the deviated side of the nose, so the chisel should be positioned lower on the deviated side to resect the difference.
- However, there are no exact formulae to calculate exactly where the chisel should be placed during the surgery relaying on the surgeon skills.
Spreader Flaps:
These are made from upper lateral cartilages that have been separated from the septal cartilage. The main advantage over spreader grafts is that there is no need to harvest cartilage from elsewhere. Rather than trimming the ULC to smoothen the new dorsal profile, the excess vertical height may be used to generate bilaterally inwardly folded cartilage flaps that are then sutured to the upper line of the dorsal septum in order to stabilize and give strength to the middle vault that has been weakened during the resection of the hump.(2)
When the ULCs are separated from the nasal septum there are three options in reconstructing the middle vault: turn the ULCs in, suture them to the nasal septum, or suture to each other over the nasal septum. In certain cases, the addition of spreader grafts can be very helpful to rebuild the middle vault more effectively.
There is a classification of spreader flaps which was presented by Dr Apaydin (4):
(A) Suturing of ULCs to the septum after septal hump removal: After rasping the bony hump, a very limited excision of the ULCs medially with some septal cartilage is done. The internal valve is not disturbed. Then the medial edges of the ULCs are simply sutured together slightly narrowing the cephalic part of the middle vault
(B) suturing of ULCs over the septum after septal hump removal: After rasping the bony hump, a very limited excision of the ULCs medially with some septal cartilage is done. The internal valve is not disturbed. Then the medial edges of the ULCs are simply sutured together slightly narrowing the cephalic part of the middle vault.
(C) Turn-in flap
(D) Suturing of ULCs to the septum and over the spreader grafts : in crooked noses
(F) Turn-in flap sutured to the spreader graft: this is used for a very marrow middle third which requires as much widening as possible.
Spreader Grafts:
First described by Sheen(5), the spreader graft is a rectangular cartilage which is positioned in between the upper lateral cartilages and the nasal septum in order to make the internal nasal valve wider.(6) The spreader graft helps to adjust dorsal deviations as well as avoid problems and complications in the mid-vault after hump removal is done.
Conclusion & advice:
- the adequate preoperative patient analysis with the understanding of the nasal aesthetic ideals and anatomy, will dictate the surgeon to select the appropriate surgical technique to have long term good result.
- Please distinguish carefully between a true hump and the illusion of a hump created by distorted anatomy as A deep radix & marked Ptotic nasal tip.
- Enhance the projection of the Tip rather than lower the dorsum
- the aesthetic and functional complications may occur immediately or years later after the surgery.
- A patient with thin skin may be at risk for visible or palpable dorsal irregularities so we advice to cover the nasal dorsum with a layer of facial at a patient with short nasal bones and long weak ULCs may be at risk for middle vault destabilization.
- The use of spreader grafts and flaps give us wonderful options but still all experienced rhinoplasty surgeons may have different thoughts and philosophies in rebuilding the middle vault.
- In a high septal deviation, the spreader graft should be longer than usual. (Figure 13)
- the spreader grafts can be used together with the spreader flaps When the ULCs are found to be weak
- in crooked noses, asymmetric noses, and revision cases, a combination of these techniques can be also useful (figure 14 )


- Strong nasal tip columellar strut to increase the strength & stability of the alar cartilage complex is essential to a have a good long-term result.
- Operative maneuvers graphical records &Good clinical photographs for understanding the patient results.
NOTE:
- During my rhinoplasty surgery, Most of the time, I prefer to suture both upper lateral cartilage together above the inserted spreader graft, to have natural smooth looking nasal dorsum, and for my conviction that this technique is better for increasing the internal nasal valve angle. (Figure 15 )
Finally, we can say that:
- Spreader grafts are excellent structural grafts
- Provide filling and stability to the middle third
- Particularly useful for filling depressions
But…
- Do not seem to improve function much
- Hard to distinguish the functional effects from
Other concomitant maneuvers e.g. turbinate & septal surgeries.
Reference:
- Bhangoo, Kulwant S. “Aesthetic rhinoplasty: avoiding unfavourable results.” Indian journal of plastic surgery: official publication of the Association of Plastic Surgeons of India 46.2 (2013): 349.
- Kovacevic, Milos, and Jochen Wurm. “Spreader flaps for middle vault contour and stabilization.” Facial Plastic Surgery Clinics 23.1 (2015): 1-9.
- Kovacevic, Milos, et al. “Options for middle vault and dorsum restoration after hump removal in primary rhinoplasty.” Facial Plastic Surgery 32.04 (2016): 374-383.
- Apaydin, Fazil. “Rebuilding the middle vault in rhinoplasty: a new classification of spreader flaps/grafts.” Facial Plastic Surgery 32.06 (2016): 638-645.
- Sheen, Jack H. “Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty.” Plastic and reconstructive surgery 73.2 (1984): 230-239.
- Kim, Leslie, and Ira D. Papel. “Spreader grafts in functional rhinoplasty.” Facial Plastic Surgery 32.01 (2016): 029-035.