Disclosure: The authors have nothing to disclose.
Keywords (4-8): Rhinoplasty, crushed cartilage, camouflage grafts, rhinoplasty augmentation, tip grafts
Abstract
Crushed cartilage grafts are a valuable option for slight augmentation and camouflage in rhinoplasty. In this chapter we describe our technique for preparing crushed cartilage in a systematic way as well as a classification system for crushed cartilage. Slightly and moderately crushed grafts are the most reliable options out of them, as cartilage viability is greatly reduced with higher levels of crushing. We include some clinical applications of these grafts. In our experience, we can get more predictable outcomes and limit graft resorption with the principles outlined.
Introduction
The use of grafts is a common practice in rhinoplasty, both for primary and for revision cases. When available, autologous cartilage is typically preferred for grafts due to its high biocompatibility, as well as low risk of infection, resorption and extrusion. Out of the different options, septal cartilage is the first-line choice for most rhinoplasty grafts. It is easily harvested both through an open or closed rhinoplasty approach, without entailing additional incisions or morbidity to secondary sites. In some scenarios, such as revision cases, there may not be enough septal cartilage, so costal or auricular cartilage may be required.
Despite the advantages of intact cartilage, there are obvious limitations when used as a dorsal onlay or camouflage graft. Intact cartilage often leaves visible and palpable edges which cause contour abnormalities. These step-offs are more prominent in thin-skinned patients, especially after edema has subsided. In order to avoid this problem, different methods of cartilage preparation have been described, such as dicing, scraping, and crushing cartilage. Other options include wrapping cartilage in different materials such as fascia, Surgicel (Johnson & Johnson Medical), fibrin glue and homologous materials. The ideal method is still a matter of debate.
Crushing cartilage is a simple procedure, however, the degree of crushing and its preparation methods are quite different among surgeons. Variable preparation methods lead to inconsistent degrees of crushing. This can result in a wide range of clinical outcomes, as the rate of cartilage resorption is proportional to the degree of mechanical trauma it sustains during crushing. To optimize the results of crushed cartilage, a consistent method is required. The purpose of this chapter is to describe a systematic way of preparing crushed cartilage as well as naming some tips and tricks for its use. We consider this a reliable way of preparing and using crushed cartilage.
Advantages and viability of crushed cartilage
As previously stated, crushing cartilage is one of the methods to avoid palpable and visible edges that can be seen with intact cartilage grafts. However, in contrast to many of its alternatives, it is quick and easy to prepare; it is easy to handle and place under the skin; and it doesn´t have additional costs, which is the case with fibrin glue or non-autologous materials.
The main disadvantage of using crushed cartilage is graft resorption, although this is not exclusive to crushed cartilage. The literature reports very variable degrees of chondrocyte viability for this technique. A possible explanation is that crushing cartilage is not a standardized process; the use of different instruments and intensities of crushing can ultimately lead to the discrepancy of results. In order to overcome the conflicting literature information and results, Cakmak proposed a classification system for crushed cartilage. This classification is useful for study purposes and also as a tool to determine the optimal level of crushing in the clinical practice. We present an updated version of Cakmak´s classification which also includes additional biomechanical characteristics (Table 1). This may aid the reader to correctly identify and obtain the appropriate level of crushing.
| Table 1. Cakmak´s Classification for crushed cartilage | |
| Degree of crushing | Appearance and biomechanical characteristics |
| Slightly crushed | The surface is softened. Recoils completely after bending. |
| Moderately crushed | Cobblestone surface. Reduced elastic strength, preserves most of its recoil after bending. |
| Significantly crushed | Cobblestone surface, may start to fragment. Flexible and malleable. Almost no recoil after bending. |
| Severely crushed | Destroyed integrity of the cartilage surface. May fracture with bending. Loses its elasticity and recoil. |
There is still an ongoing debate about the viability of crushed cartilage. Despite the discrepancies between publications, it is generally accepted that cartilage survival is reduced with greater degrees or levels of crushing. The senior author (O.C.) has comprehensively analyzed the subject by conducting a series of in vitro, animal, and clinical studies to determine the viability of crushed cartilage using a standardized process and classification system. Prior to these studies, there were only a few descriptions about crushed cartilage viability. According to his published results, as well as to his ongoing personal experience, crushed cartilage is a valuable graft in rhinoplasty when limited to slight and moderate crushing levels (Table 1). Clinically he has observed that slightly crushed grafts survive just as well as intact cartilage grafts, while moderately crushed grafts have a very low resorption rate. In contrast, significantly and severely crushed cartilage have high risk of resorption. Subsequent publications from other authors have reproduced some of these results and also support the use of slightly and moderately crushed cartilage grafts.
Applications and limitations
Crushed cartilage is mainly used for slight augmentation and camouflage. We emphasize that as a single technique, its use should be reserved for small irregularities and depressions, which are addressed by placing the crushed cartilage in one or in multiple layers. Due to its limited thickness, crushed cartilage grafts are not ideal for correcting major depressions. In case of moderate or severe deformities, it can be placed on top or on the margins of intact cartilage grafts. This can help as a final touch-up to smooth out any small remaining irregularities and edges, thus providing improved aesthetical results. Clinically we consider it a very valuable option to augment or camouflage problems in the following areas:
- Radix
- Nasal dorsum
- Nasal side walls
- Nasal tip
- Columella
- Soft tissue triangle
When using crushed cartilage grafts, slightly and moderately crushed levels are generally preferred due to their low resorption rates. We exceptionally use significantly and severely crushed cartilage to soften the edges of remaining irregularities on the nasal tip, especially in patients with thin skin and revision cases with poor skin quality; they can also be used for contouring of the columella and soft tissue triangle. We avoid using significantly or severely crushed cartilage for augmentation purposes. It is also important to note that crushed cartilage should not be relied on for structural support.
How to prepare and apply crushed cartilage
The surgeon must first evaluate if a specific problem can be addressed with crushed cartilage and then estimate the amount that will be needed. Based on this, the planned amount of cartilage is harvested, usually from the septal cartilage. Auricular and rib cartilages can also be used when no septal cartilage is available, but have some additional drawbacks. Auricular cartilage is more delicate and can be easily overcrushed, while rib cartilage is stiffer and can be shattered with the crushing process.
After harvesting the cartilage, the remaining perichondrium and bony fragments must be removed from the cartilage prior to crushing. The intact cartilage pieces that will be crushed are then shaved to a homogenous thickness of no more than 3 mm (Figure 1). This is an important step, as an irregular thickness will lead to overcrushing at the thicker parts of the grafts. Microscopically, these excessively crushed areas have an increased proportion of nonviable cells, which may lead to increased graft resorption.
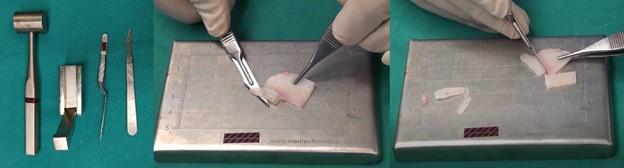
For crushing, the senior author uses a Cottle cartilage crusher (model 523900; Karl Storz GmbH & Co, Tutlingen, Germany). The process is straightforward. The desired piece of cartilage, that was previously trimmed to a 2-3 mm thickness, is placed on the crusher. Sequential hits are applied until the desired level of crushing is obtained (Figure 2). Cakmak’s Classification is based both on the appearance and biomechanical properties of the crushed cartilage graft (Figure 3 and Video 1). The same level of crushing can be obtained with a few forceful hits as well as with a greater number of light hits. We recommend using a greater number of light hits as this is a more controlled way of getting the desired crushing level.


Video 1
In order to obtain grafts with the appropriate levels of crushing (slight and moderate), we recommend the following keypoints:
- The initial cartilage should have a homogeneous thickness of no more than 3mm
- The crushed graft should have a cobblestone or alligator skin appearance
- The graft should maintain its structural continuity; it shouldn´t be fragmented or destroyed
- Most of the elasticity and recoil should be preserved when palpating and flicking the graft
- It is easier to obtain these results with consecutive light hits
After the cartilage is crushed, it is placed in saline solution and then applied with a toothless bayonet forceps. Slightly and moderately crushed cartilages are easy to handle and place under the skin. They can be placed without suture fixation on the dorsum, radix, sidewalls, and supratip. These should be placed at the end of the rhinoplasty, just before the closure of incisions to prevent graft displacement. We only recommend suture fixation when used as tip grafts. Correct positioning can be confirmed by both, direct visualization, and by palpating the skin of the nasal pyramid. At the end of the procedure, we recommend taping in a caudal to caudal direction to retain the grafts in place. We avoid overcorrecting any irregularities or depressions. In case of mild unintentional overcorrection, we recommend a gentle finger massage over the graft during the first few weeks postoperatively.
Clinical examples
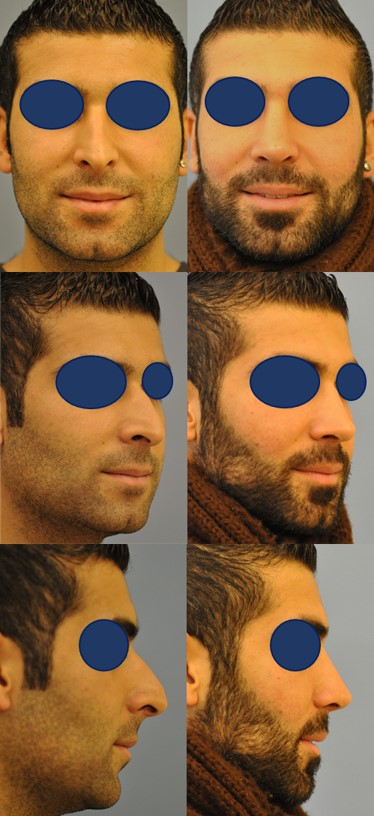
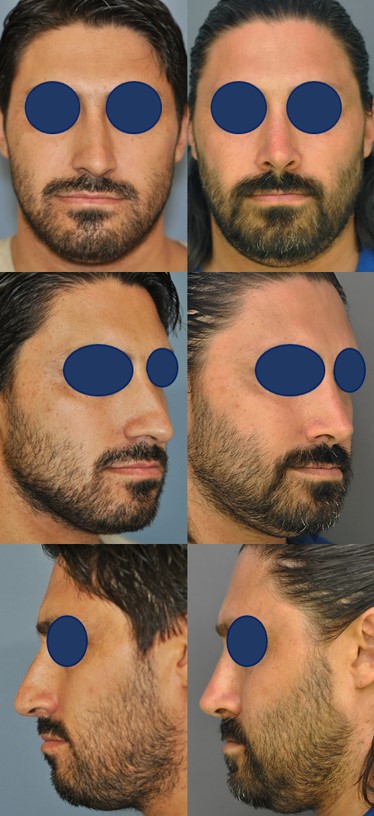
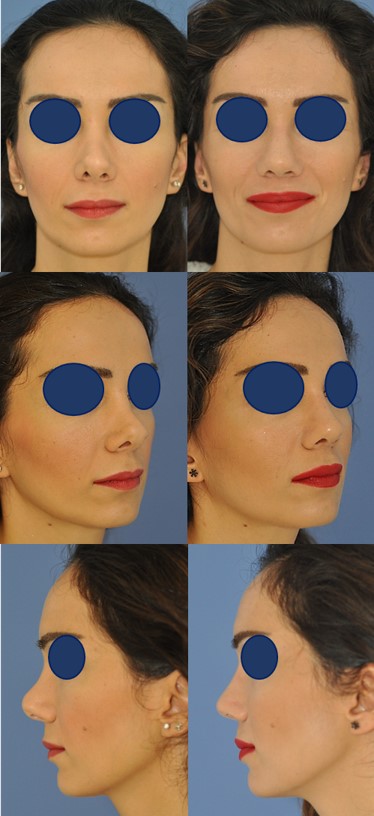
We present five cases where crushed cartilage grafts were used for camouflage and/or slight augmentation at the end of the rhinoplasty, just before closing the incisions. Figures 4, 5, and 6 are primary rhinoplasty cases. Figures 7 and 8 correspond to revision rhinoplasty cases.


Conclusion
We have yet to find a perfect grafting solution. Among the different grafts, crushed cartilage is a very valuable option for slight camouflage and augmentation. The use of a simple and reproducible method such as the one described is required to obtain results as consistent as possible. Cakmak´s Classification is a useful tool to prepare crushed cartilage. Although there is always a possibility of graft loss, resorption is rare with slightly and moderately crushed grafts, and have yielded good long-lasting results in the senior author´s practice. Based on studies and clinical experience, we can recommend using slightly and moderately crushed cartilage. They are effective and reliable options to correct depressions and irregularities in rhinoplasty surgery.
References
- Cakmak O, Altintas H. A Classification for degree of crushed cartilage. Arch Facial Plast Surg. 2010;12(6):435-436. doi:10.1016/j.jcms.2010.03
- Cakmak O, Buyuklu F. Crushed cartilage grafts for concealing irregularities in rhinoplasty. Arch Facial Plast Surg. 2007;9(5):352-357. doi:10.1001/archfaci.9.5.352
- Cakmak O, Bircan S, Buyuklu F, Tuncer I, Dal T, Ozluoglu LN. Viability of crushed and diced cartilage grafts. Arch Facial Plast Surg. 2005;7(1):21. doi:10.1001/archfaci.7.1.21
- Cakmak O, Buyuklu F, Yilmaz Z, Sahin FI, Tarhan E, Ozluoglu LN. Viability of cultured human nasal septum chondrocytes after crushing. Arch Facial Plast Surg. 2005;7(6):406. doi:10.1001/archfaci.7.6.406
- Cakmak O, Buyuklu F. Survival of diced cartilage grafts: an experimental study. Plast Reconstr Surg. 2006;118(7):1658; author reply 1658-9. doi:10.1097/01.prs.0000244301.66034.74
- Cakmak O. Crushed Cartilage Grafts: Is overcorrection necessary? Arch Facial Plast Surg. 2008;10(6):428. doi:10.1001/archfaci.10.6.428-a
- Buyuklu F, Hizal E, Yilmaz Z, Sahin FI, Cakmak O. Viability of crushed human auricular and costal cartilage chondrocytes in cell culture. J Cranio-Maxillofacial Surg. 2011;39(3):221-225. doi:10.1016/j.jcms.2010.03.013
- Buyuklu F, Cakmak O. Histological analysis of human diced cartilage grafts. Plast Reconstr Surg. 2007;120(1):348-349. doi:10.1097/01.prs.0000264563.48652.a6
- Hizal E. Buyuklu F, Ozer O, Cakmak O. Effects of different levels of crushing on the viability of rabbit costal and nasal septal cartilages. Plast Reconstr Surg. 2011;128(5):1045-51. doi: 10.1097/PRS.0b013e31822b6651
- Peer LA. The neglected septal cartilage graft, with experimental observations on the growth of human cartilage grafts. Arch Otolaryngol 1945;42: 384- 396. doi:10.1001/archotol.1945.00680040504008
- Verwoerd-Verhoef HL, Meeuwis CA, van der Heul RO, Verwoerd CD. Histologic evaluation of crushed cartilage grafts in the growing nasal septum of young rabbits. ORL. 1991;53(5):305-309. doi:10.1159/000276234
- Stoksted P, Ladefoged C. Crushed cartilage in nasal reconstruction. J Laryngol Otol. 1986;100(8):897-906. doi:10.1017/s0022215100100295
- Yilmaz S, Ercocen AR, Can Z, Yenidunya S, Edali N, Yormuk E. Viability of diced, crushed cartilage grafts and the effects of Surgicel (oxidized regenerated cellulose) on cartilage grafts. Plast Reconstr Surg. 2001;108(4):1054-1060; discussion 1061-1062. doi:10.1097/00006534-200109150-00040
- Vuyk H, Adamson P. Biomaterials in rhinoplasty. Clin Otolaryngol Allied Sci. 1998;23(3):209-217. doi:10.1046/j.1365-2273.1998. doi: 10.1046/j.1365-2273.1998.00133.x
- Bujia J. Determination of the viability of crushed cartilage grafts: clinical implications for wound healing in nasal surgery. Ann Plast Surg. 1994;32(3):261-265.
- Breadon GE, Kern EB, Neel BH. Autografts of uncrushed and crushed bone and cartilage. Arch Otolaryngol 1979;105(2): 75- 80. doi:10.1001/archotol.1979.00790140021004
- Rudderman RH, Guyuron B, Mendelsohn G. The fate of noncrushed and crushed autogenous cartilage in the rabbit model. Ann Plast Surg 1994;32(3):250-254. doi:10.1097/00000637-199403000-00004
- Garg R, Shaikh M, Foulad A, Wong B. Chondrocyte viability in human nasal septum after morselization. Arch Facial Plast Surg. 2010;12(3):204-206. doi:10.1001/archfacial.2010.35
- Hamra ST. Crushed cartilage grafts over alar dome reduction in open rhinoplasty. Plast Reconstr Surg. 1993;92(2):352-356. doi:10.1097/00006534-199308000-00026
- Hamra ST. Crushed cartilage grafts over alar dome reduction in open rhinoplasty. Plast Reconstr Surg. 2000;105(2):792-795. doi:10.1097/00006534-200002000-00052
- Sajjadian A, Rubinstein R, Naghshineh N. Current status of grafts and implants in rhinoplasty: part I. Autologous grafts. Plast Reconstr Surg. 2010;125(2):40e-49e. doi:10.1097/PRS.0b013e3181c82f12
- Sajjadian A, Naghshineh N, Rubinstein R. Current status of grafts and implants in rhinoplasty: part II. Homologous grafts and allogenic implants. Plast Reconstr Surg. 2010;125(3):99e-109e. doi:10.1097/PRS.0b013e3181cb662f
- Jang YJ, Moon BJ. State of the art in augmentation rhinoplasty. Curr Opin Otolaryngol Head Neck Surg. 2012;20(4):280-286. doi:10.1097/MOO.0b013e328354b390
- Yu MS, Kim BH, Kang SH, Lim DJ. Combined use of crushed cartilage and fibrin sealant for radix augmentation in Asian rhinoplasty. Plast Reconstr Surg. 2015;135(2):293e-300e. doi: 10.1097/PRS.0000000000001114.
- Boccieri A, Marianetti TM, Pascali M. Crushed cartilage: a rescue procedure in rhinoplasty. J Craniofac Surg. 2018;29(3):614-617. doi: 10.1097/SCS.0000000000004333