Abstract
The deviated nose constitutes the most severe and complex deformation of the nasal septum. Deviation of the dorsal portion of the septum not only gives rise both to functional problems and to asymmetry and aesthetic deformity, often with a marked social impact, but also proves one of the most difficult conditions to correct because in most cases it involves the supporting L-shaped structure, which must always be preserved. At the same time, however, the effects of surgical correction tend to be nullified in time by “cartilaginous memory,” understood as the tendency of the cartilage to revert to its original shape, which is not easy to eliminate and does not disappear over time. At the moment, there are essentially three surgical techniques in the literature capable of providing a definitive solution to the dorsal deviation of the nasal septum that causes the condition of deviated nose: 1) external reshaping of the septum; 2) the monolateral or bilateral spreader graft; 3) the septal crossbar graft.
The pathological anatomy of the deviated nose
Deviation of the nasal septum can be linear, C-shaped or S-shaped with respect to the median line (figs. 1, 2 and 3).



The condition can regard the whole of the nasal pyramid or be limited with varying degrees of deformity to the upper, middle or lower portion of the nasal dorsum. In addition to the dorsal septum, deviation of the nasal septum can also involve the basal and median septal regions, the perpendicular plate of the ethmoid bone, the vomer, the anterior nasal spine and the maxillary crest. Deformity of the upper portion of the dorsum is determined by deviation of the nasal bones, which can be symmetrical or asymmetrical in shape, size and position, with respect to the median line. In the middle third, support for the nasal pyramid is provided by the dorsal-most portion of the septal cartilage and the two lateral cartilages, which present anatomical continuity.
The cutaneous and subcutaneous covering of this region is so thin that even the slightest irregularity or asymmetry can show through. While deviation of the middle third is related essentially to the dorsal septum, the lateral cartilages can also play an important role, often proving to be depressed on the concave side of the deviation and reducing the angle of the internal nasal valve to below the physiological values of 10-15°. The resulting stenosis of the internal nasal valve aggravates the respiratory difficulties already caused by the septal deviation. Deformity of the lower third can be due to deviation of the caudal septum or nasal spine or to dislocation of the basal septum from the maxillary crest.
The infero-caudal portion of the septum can be dislocated in one of the two nostrils so as to obstruct airflow. This portion normally provides support for the nasal tip through ligamental connections with the medial crura and domes. If the caudal septum is severely deviated, it can no longer perform this important function and the nasal tip may lose projection through lack of the necessary support. This is often associated with asymmetry of the lateral crura of the alar cartilages with deviation and hypertrophy of one side with respect to the other. The medial crura can also present varying degrees of deviation. Nor should it be forgotten that the cutaneous covering and the SMAS adapt to deviation and the asymmetric development of cartilages by means of a mechanism of expansion or contraction and can therefore present differences in shape and thickness.
From the physiopathological viewpoint, it is important to emphasize the presence in the deviated nose of dislocating forces of an intrinsic or extrinsic nature that act on the cartilaginous portion of the nasal septum. These are the cause of the septal deviation and can lead to relapse if they are not brought into balance. The extrinsic forces acting on the septum are those generated by deviated nasal bones and connections with the lateral cartilages, the vomer, the ethmoid bone and the maxillary crest. The intrinsic forces are instead due to mechanisms of reciprocal intracartilaginous stress caused in turn by polysaccharide-protein complexes associated with collagenic fibers. They constitute an inherent tendency of the cartilage to revert to the original shape after correction. It is precisely as a result of this “memory” and/or failure to eliminate all of the extrinsic dislocating forces that a result which appears more than satisfactory in the immediate post-operative phase can prove a failure a few months after the operation due to relapse.
Correction of the deformity
Deviation of the upper third of the nasal dorsum (nasal bones) usually presents no great problem and can nearly always be solved by means of basal, median and – if necessary – intermediary and/or transversal osteotomies. Moreover, since the reshaping is carried out on bone, the result remains stable once a fibrocartilage callus has formed.
The greatest difficulties arise in the correction of deviation of the middle and lower dorsal portions. Even though it is possible to remove most of the nasal septum, it is essential to preserve an L-shaped dorsal structure of support, and the problems arise because this also proves crooked in such cases. The countless techniques described in the literature are indicative of just how important and difficult it is to correct this deformity. The swinging door technique described by Metzenbaum and modified by Seltzer involves the resection of a vertical strip of septal cartilage followed by a longitudinal incision of the basal septum along the nasal floor.
The septal cartilage can thus be mobilized, swung back (like a door) into a median position, and secured to the columella. Maliniac, Becker, Converse, Rees and others have suggested weakening the cartilage by means of multiple incisions in order to break the spring of its “memory” and straighten the nasal septum. Lawson and Reind consider it sufficient to make incisions all the way through the cartilage on the concave side of the deviation and leave the mucoperichondrium of the convex side intact. Jost’s “spiral” incision exemplifies the techniques aimed at weakening the septum with a view to its lasting realignment. In practice, many of the techniques described in the literature involve morsellization, incisions and resections of cartilaginous wedges in order to counter the cartilaginous memory. Very often, however, they result in relapse over time or collapse of the L-shaped supporting structure due to excessive weakening.
As things now stand, three techniques are considered capable of providing a lasting solution to dorsal deviation of the septum.
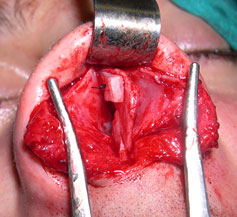
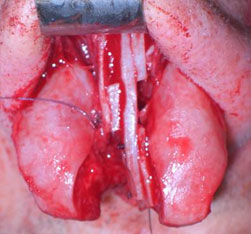
The first is the external septoplasty originally described by Galloway and Fomon, and subsequently used by Converse, Cottle, Rees, Sulsenti, Palma and Gubisch. The latter suggests complete removal of the septum, reshaping with incisions and sutures to create a straight structure, and reinsertion between the two flaps of the mucoperichondrium. A portion of the perpendicular plate of the ethmoid bone can be sutured to one side of the “neo-septum” before insertion so as to give it greater straightness and strength (figs. 4-5).
The technique offers a brilliant and radical solution to the problem of the deviated nose but requires particular skill in the phase of septum insertion in order to avoid irregularity at the rhinion. Gubisch himself recommends the systematic use of a suture to hold the lateral cartilages and the reshaped dorsal septum in place. This is very easy to perform by means of the open approach and reduces the sequela of dorsal sagging from 1.5% to 0%.


The second is the use of spreader grafts. Toriumi and Ries suggest that the placement of a spreader graft on the concave side in C-shaped deviations can serve both to improve the respiratory function and to harmonize the brow-tip aesthetic line. While Rohrich is also in favor of the monolateral technique, Guyuron proposes the use of bilateral spreader grafts in order to provide stronger opposition to the cartilaginous memory. Finally, Byrd suggests the use of a septal extension graft in the same position as the spreader graft on the concave side so as to make control over the projection and rotation of the tip possible as well.
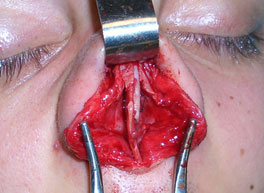
The spreader graft acts as a splint on the dorsal septum while exerting lateral pressure on the lateral cartilages (figs. 6-7).

In the case of a C-shaped deviation, the spreader graft should be inserted on the concave side so as to realign the deviated axis of the lower two thirds of the nasal pyramid (figs. 8-9).


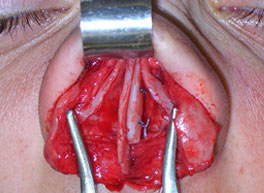
In the case of linear deviation, it should instead be inserted on the opposite side, i.e. the side where there is a gap between the dorsal septum and the lateral cartilage (figs. 10-11).

While spreader grafts can be inserted by means of both the closed and the open approach, the latter provides a clearer view of the nasal structures and makes the operations of positioning and suturing easier and more precise. Crucial importance attaches in fact to securing the spreader graft not only at the septal angle but also in the most cephalic position, where suturing proves extremely difficult with the closed approach but comparatively easy with the open (figs. 12-13).

Moreover, the open approach makes it possible to suture the lateral cartilages to the septum or the spreader grafts previously placed in position. This surgical phase is important and should always be performed in order to avoid possible “curling” of the lateral cartilages and the resulting post-operative deformity.
The third technique capable of correcting even major deviations of the dorsal septum with definitive and lasting success is the septal
crossbar graft, introduced in 2003, which rests on the same philosophy as the use of spreader grafts in septal correction. Both grafts are designed to strengthen the dorsal pillar of the L-shaped structure so that it can be straightened and reshaped with multiple incisions with no fear of excessive weakening.
The surgical technique begins with the execution of a classic septoplasty, leaving an L-shaped structure at least 15 mm in thickness in place and harvesting a straight strip of septum measuring 3–6 mm in height, 15–25 in length and 1–3 in thickness. If no septal cartilage is available, use can be made of a strip of the perpendicular plate of the ethmoid bone. Auricular cartilage is instead not suitable for the purposes of this technique because of its curvature and comparative lack of strength. Before insertion of the graft, a series of incisions must be made in the area of the two pillars, dorsal and caudal, of the L-shaped structure. Three incisions are sufficient for each pillar, one on the inside and two on the outside at the points where the deviation is greatest. The graft should be placed in position on the dorsal septum before making the incisions so that the correct positions can be identified for the latter.
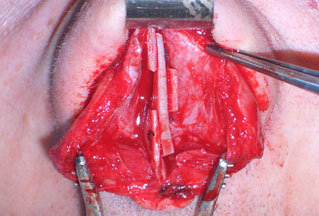
The crossbar graft is then inserted between the two incisions of the dorsal pillar on the concave side of the deviation (fig. 14).
The lower portion of the graft can be given a more or less accentuated wedge-like shape so as to adapt it to the scale of the deviation by adjusting the gap of the central part of the L structure. Once the crossbar graft is in position, it should be secured with two sutures of Vicryl 5.0. A third suture can be used to secure the central section if greater stability is required. Finally, the lateral cartilages must be sutured to the nasal septum (figs. 15, 16).

The insertion of the septal crossbar graft entails use of the open approach because of the need both for the maximum visibility and precision and for sutures that prove impossible with the closed approach. The septal crossbar graft can be regarded as an intraseptal spreader graft in that it is lodged between the two parallel incisions in the dorsal septum. This procedure makes it possible to obtain twice as much space between the septum and the lateral cartilages as with a single spreader graft.
It is currently the technique best capable of correcting the most severe septal deviations and countering the effects of the cartilaginous memory. It also plays an important part in improving respiratory functionality by acting as a spreader graft to create a correct angle bilaterally at the level of the internal nasal valve. In the case of severe deviations of the nasal dorsum, this angle is usually below 10°, above all on the concave side, where the lateral cartilage is depressed.
It should in fact be noted that depression of the lateral cartilage on the concave side is often considered an ineradicable blemish even in cases of deviated nose brilliantly solved by means of other techniques. This is due to the difficulty of reshaping these cartilaginous structures of reduced thickness and consistency. At the same time, the onlay grafts used by some authors to mask this residual deformity often prove ineffective both because of resorption problems and because they lead to collapse of the lateral cartilage. The septal crossbar graft instead exerts direct upward pressure that supports and repositions the lateral cartilage, which thus becomes capable of supporting any small onlay grafts that might prove necessary (fig. 17).
While the procedures described here have made it possible to obtain excellent results in the treatment of the deviated nose in recent years, they can be regarded at most as marking an important point of transition.

Surgery of the deviated nose is in fact currently moving from the somewhat empirical approach of the past to one that is more objective and rigorously scientific, and there is probably still a long way to go, given that the problems of this pathology have yet to be completely solved. A highly self-critical attitiude is always required in the assessment of results.
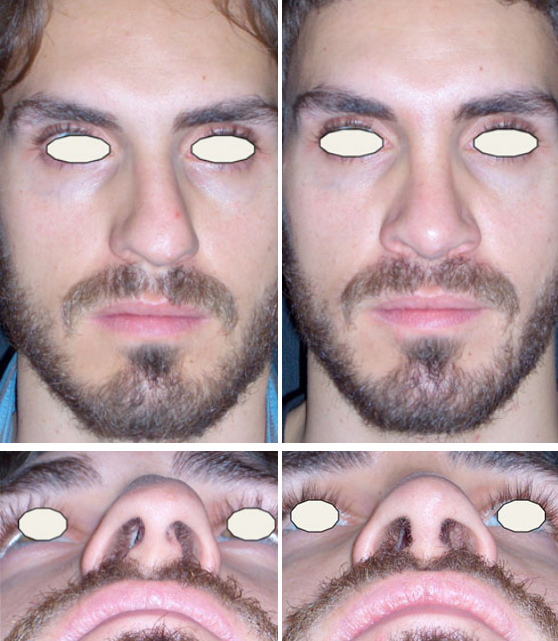
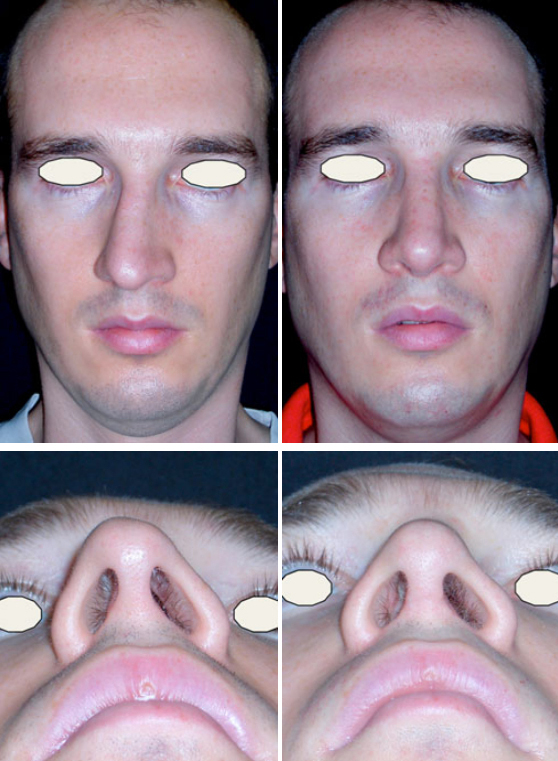
The correction of crooked nose is illustrated in three cases where the treatment was performed with three different procedures.
Clinical Cases

References
Boccieri A, Pascali M. Septal crossbar graft for the correction of the crooked nose. Plast Reconstr Surg 2003; 111: 629-638.
Toriumi DM, Ries WR. Innovative surgical management of the crooked nose. Facial Plast Clin North Am 1993; 1: 63-78.
Boccieri A. Evolution of the septal crossbar graft technique. Facial Plast Surg 2006; 22 (4): 255-65.
Gubisch W. Twenty-five years experience with extracorporeal septoplasty. Facial Plast Surg 2006; 22 (4): 230-9.
Mackay IS. The deviated nose. Fac Plast Surg 1986; 3: 253-265.
Pirsig W. Rhinoplasty and the airway in children. Facial Plast Surg 1986; 3: 225-234.
Tardy ME. Rinoplastica: Lo stato dell’Arte. Vol. II. Naples: EdiSes S.r.l., 1999.
Byrd HS, Salomon J, Flood J. Correction of the crooked nose. Plast Reconstr Surg 1998; 102: 2148-2157.
Pontius AT, Leach JL. New Techniques for management of the crooked nose. Arch Facial Plast Surg 2004; 263-266.
Byrd HS. The crooked nose; an algorithm for repair. Presented at 17th Annual Dallas Rhinoplasty Symposium 2000; 239-242.
Costantian MB, Clardy RB. The relative importance of septal and nasal valvular surgery in correcting airway obstruction in primary and secondary rhinoplasty.
Plast Reconstr Surg 1996; 98: 38-53.