Saddle nose is a clearly visible depression of the nasal dorsum that impairs the aesthetic harmony of the face and proves particularly unattractive in men and in those of Latin or Mediterranean ethnicity in general.
This deformity is frequently accompanied by other impairments such as internal nasal valve incompetence, loss of tip support and columellar retraction. An increase in nasal resistance is also observed in these cases and patients often complain of difficulty in nasal respiration.
The appraisal and possible correction of saddle nose must therefore be undertaken with a global approach to the nose and careful study of all the nasal structures.
Causes Of Saddle Nose
While saddle nose can be congenital, it arises in the great majority of cases as the result of various causes, including the following:
- facial trauma
- hematoma of the septum
- cocaine abuse
- some rare diseases (e.g. Wegener’s granulomatosis, leprosy and autoimmune chondritis)
- surgical operations
Traumatic Saddle Nose
In children
Nasal trauma proves particularly serious in children. Even when the fracture appears to have been appropriately treated, the damage to structures can impair the growth of the nasal framework in such a way as to result in permanent deformity that emerges fully in adulthood.
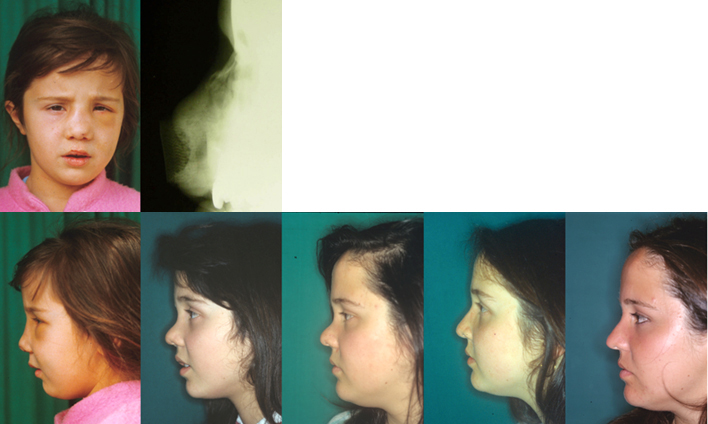
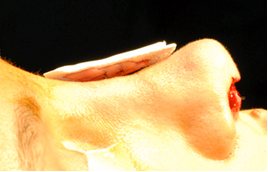
Above: displaced fracture of nasal bones.
Below: evolution of the lesion over the years.
From left to right: at the moment of the trauma at the age of 3, age 10, age 13, age 14 after reconstruction surgery with grafts of auricular cartilage, and age 17.
In adults
In the event of trauma with depressed fracture of the nasal bones, correct reduction and containment of the fracture generally ensures successful healing with no deformities. In the case of repeated traumas, as happens for example with those who practice boxing, the fragmentation and often resorption of nasal bones is such as to prevent repositioning of the fragments and the result is permanent saddle nose with the point of greatest depression generally located in the upper third of the nasal pyramid.
Saddle Nose Caused By Hematoma Of The Septum Or Use Of Local Vasoconstrictors
Both hematoma of the septum, if not promptly treated, and chronic use of vasoconstrictors can lead through different mechanisms to resorption of the quadrangular plate. When the lack of cartilage becomes particularly extensive, the septum can no longer provide a supporting structure for the nasal dorsum. The saddle nose deformity that can result in this case has its point of greatest depression in the middle vault and is often accompanied by columellar retraction.


Iatrogenic Saddle Nose
In a series of 157 revision rhinoplasties carried out by the author in the last 5 years, 43 (27.3%) included correction of a more or less accentuated condition of saddle nose. It can be deduced that excessive resection is one of most frequent pitfalls for surgeons in the correction of nasal hump. Use of the scalpel increases the risk of excessive resection with respect to other methods and in particular to rasping, which proves unquestionably safer and more prudent due to the gradual nature of the action and hence greater control over the degree to which the dorsum is lowered. On the other hand, use of the rasp or file can lead to overestimation of how much material has been removed and hence to the opposite risk of not eliminating the hump completely.
Moreover, as a result of the change in taste that has taken place since the 1980s, many of the patients – especially those of the female sex – who underwent rhinoplasty during the 1960s in accordance with the aesthetic and surgical canons of the time now want another operation in line with the more modern ideas of beauty. The small, upturned and slightly concave Brigitte Bardot nose fashionable in the 1960s and ’70s has now given way to a straight or at most minimally curved nose that is regarded as more “natural” on the whole.
Rhinoplasty For Saddle Nose
While the surgical options for correction of saddle nose vary for each individual case, the open approach is now used for the insertion of grafts.
In addition to analysis of the other associated dimorphisms that are nearly always present in secondary cases, the elements to be assessed most specifically are the following:
- degree of depression
- existence or otherwise of septal support
- presence of open roof
- presence of columellar retraction
The first element to be assessed is the degree of depression.
1. Minimal-slight saddle nose
Some patients of the male sex reject even slight concavity of the nasal dorsum because it gives them an effeminate appearance. Some female patients also find that this makes their nose look artificial or clashes with their ethnic characteristics.
Autologous crushed cartilage can be used in cases where the dorsal depression is minimal and a graft of no more than 1–2 mm in thickness is required. As this material has been crushed and therefore lost its structure, either septal or auricular cartilage can be used depending on availability.
Expanded polytetrafluoroethylene (EPTFE) in sheets of 1 or 2 mm in thickness constitutes a valid alternative. This material (Gore-Tex soft-tissue patch) is completely biocompatible and so soft as to adapt perfectly to the nasal dorsum. A single 1 mm sheet can be implanted or, if necessary, two sheets sutured together. It has the advantage over cartilage that the nasal dorsum assumes a perfectly uniform appearance and the graft is completely undetectable, even by touch.
A simple way to determine the shape and size of the Gore-Tex graft is to draw the boundary of the defect on the skin in methylene blue and place the material in contact with this outline while still wet so that it can then be cut accordingly. If the pouch created on the nasal dorsum is the right size, the graft will require no sutures. Care is required in inserting the graft to make sure that it lies flat in the prepared pouch with no creasing or curling.

2. Medium saddle nose
The use of Gore-Tex alone can prove insufficient when the nasal dorsum has to be raised by more than 2 mm. My preference in such cases is for a composite graft of autologous cartilage, from the septum or the auricular concha, covered by one or two layers of Gore-Tex. While the cartilage supplies the volume, the layer of EPTFE covers its edges so as to make the graft undetectable. The cartilage and Gore-Tex are attached to one another with sutures of 6.0 nylon before insertion.
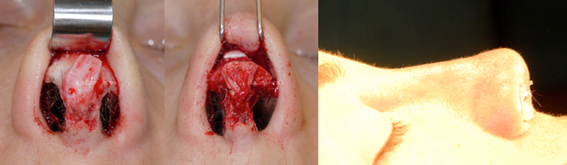
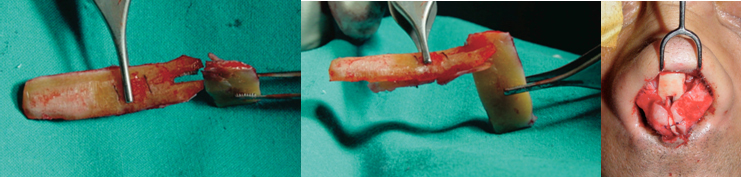
Left: probable imperfect Goldman’s tip with lateral crura of the lower lateral cartilages not identifiable.
Center: reconstruction with dorsal graft and shield graft.
Right: immediate intraoperative result.

3. Severe saddle nose
Severe saddle nose presents problems that are not exclusively aesthetic but also respiratory due to the involvement of the nasal septum in most cases. Reconstruction of the nasal septum, which is a key structural element for support of the nasal dorsum, is crucial in the correction of severe saddle nose. The same holds for support of the nasal tip, which is often under-projected or flattened.
As a result, reconstruction requires grafts of material with the following characteristics:
- abundant availability
- sufficient rigidity to counter the forces of cicatricial retraction
- lasting stability
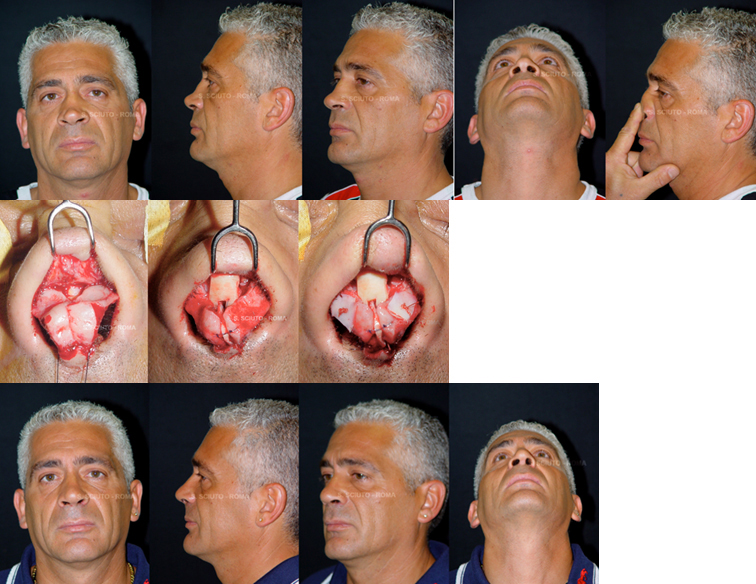
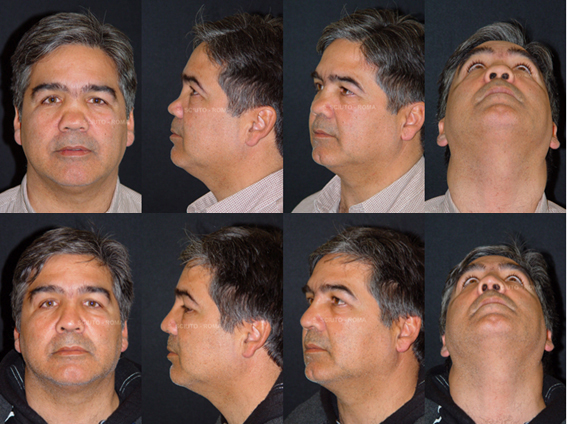
Above: saddle nose caused by an operation that demolished the nasal septum during adolescence. Lack of support for the nasal dorsum due to absence of the septum.
Middle, from left to right: lateral concave crura; reconstruction of supporting L-shaped structure consisting of caudal neo-septum and dorsal graft; overlay grafts to correct concavity of the lateral crura.
Below: postoperative view.
For these reasons, costal cartilage is preferable to both septal (which is seldom available) and auricular (which is soft and flexible).
Suitably shaped costal cartilage permits the effective reconstruction of an L-shaped structure providing adequate support for the nasal dorsum and tip as well as any further components of the nasal framework that may be required.
The distal extremity of the dorsal part of the graft is forked so as to form a joint with the septal part.
The two elements are secured to one another with non-absorbable sutures. The element constituting the septal part of the L-shaped structure is attached with absorbable sutures to the medial crura of the lower lateral cartilages. The dorsal part can be immobilized with transcutaneous sutures to be removed on the seventh day.
This type of graft fills the dorsal depression while providing adequate support for the nasal tip and correcting any columellar retraction present.
Projection Of The Nasal Tip In Saddle Nose Correction
The reconstruction of dorsal support with an L-shaped structure may prove insufficient to ensure the right degree of tip projection and definition, which requires an adequate difference in height between the maximum projection of the cartilaginous dorsum and the maximum projection of the neo-tip. In the case illustrated in fig. 12, the L-shaped structure of costal cartilage with the dorsal graft on top of the columellar fails to provide correct projection of the tip.
If an attractive tip is to be obtained, it is necessary to complete the reconstruction with a graft that increases the degree of its projection, such as a columella shield graft expanding upward and surmounted if necessary by a further umbrella graft. The difference in height between the end of the neo-tip and the dorsum must be at least 5–7 mm, especially in revision rhinoplasty.
Conclusions
The various techniques described and the different materials for grafts are selected in relation to the specific characteristics of the nose in each case. Filling the dorsal depression with a strip of PTFE or crushed cartilage simply laid on the dorsum is a minimal approach suitable for a slight degree of saddle nose. It has the advantage of being a quick and comparatively non-invasive procedure with minimal risk of complications.
Gore-Tex has always proved immune to infection or extrusion when correctly applied, which means only for the dorsum (never for the tip) and in thicknesses of no more than 2 mm. Cartilage (septal or auricular) or composite grafts must be used in cases where greater thickness is required.
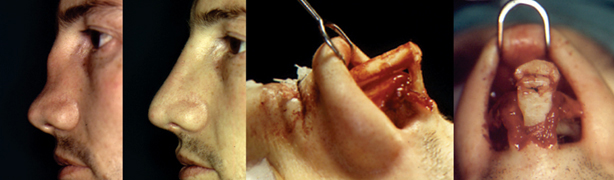
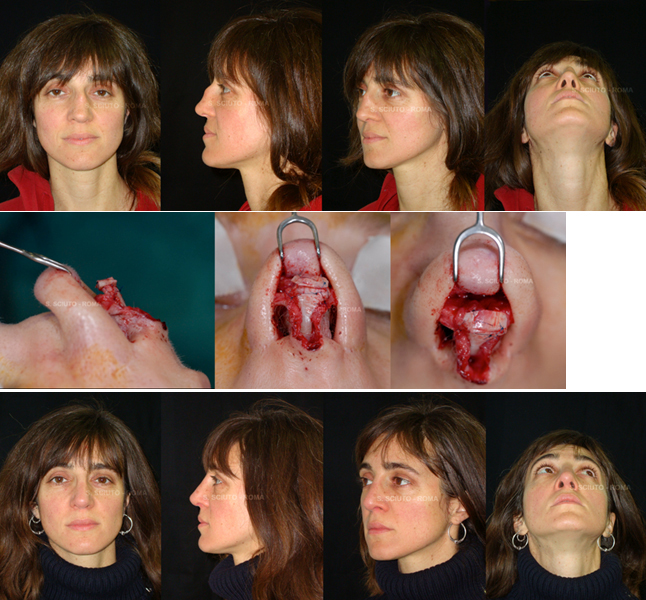
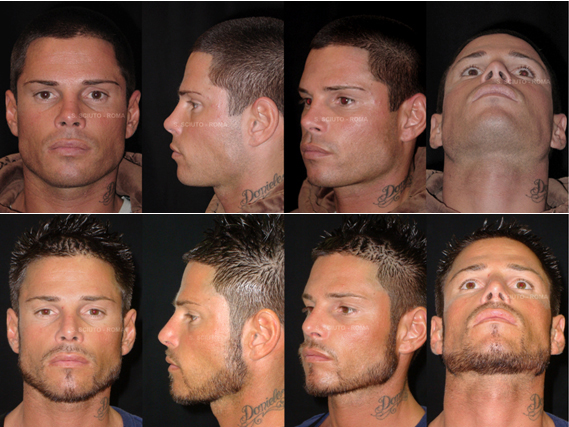
Above: saddle nose as the result of septoplasty with complications leading to almost total resorption of the septum and collapse of the cartilaginous vault.
Middle: reconstruction of an L-shaped structure to support the dorsum completed with grafts to ensure the projection and definition of the tip.
Below: the end result obtained by balancing the profile through reconstruction of the cartilaginous dorsum and excision of the osseous dorsum
Costal cartilage is used when the material has to be not only abundant but also tough and rigid enough to counter the forces of cicatricial contraction, which are very strong and prolonged in tissues already operated on once, twice and often even more times.