Abstract
Deviated nose is one of the most difficult problems to correct even for experts of rhinoplasty. To correct the deviated nose, preoperative diagnosis and examination are as important as surgical techniques. After precise preoperative examination and planning, proper surgical techniques should be applied according to anatomical location and type of deviation to correct the deviation. In this review, the authors introduce methods for successful correction of deviated noses, including personal tips.
Introduction
Deviated nose is a common problem encountered in rhinoplasty, and it is one of the most challenging problems to manage, even for experienced surgeons1. Causes of the deviated nose include congenital deformity, injury during childbirth, trauma, complication of surgery, and infection.. Among many causes, external nasal trauma is the most important etiology. Traumatized bone can develop secondary deformity of the external nose during the healing process. Nasal trauma that occurred at infancy to early childhood may stay hidden and can be manifested as an obvious nasal deformity with the rapid facial growth during adolescence.
Classification
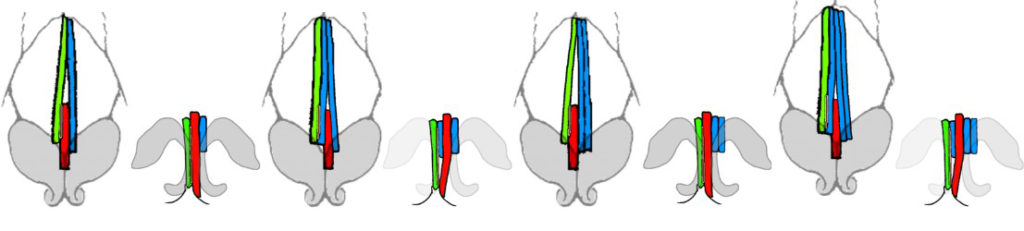
For more accurate diagnosis and treatment, some studies proposed classification to categorize deviated noses2,3. The senior author (Y.J. Jang) categorizes deviated noses into five different types4. This classification system divides the nasal dorsum into two portions: bony and cartilaginous part (figure 1).
- Type 1: Straight tilted bony pyramid and cartilaginous vault in the opposite direction
- Type 2: Straight tilted bony pyramid with bent cartilaginous vault (concavely or convexly)
- Type 3: Straight bony pyramid parallel to the facial midline and tilted cartilaginous vault
- Type 4: Straight bony pyramid parallel to the facial midline and bent cartilaginous vault
- Type 5: Straight tilted bony pyramid and cartilaginous vault in the same direction
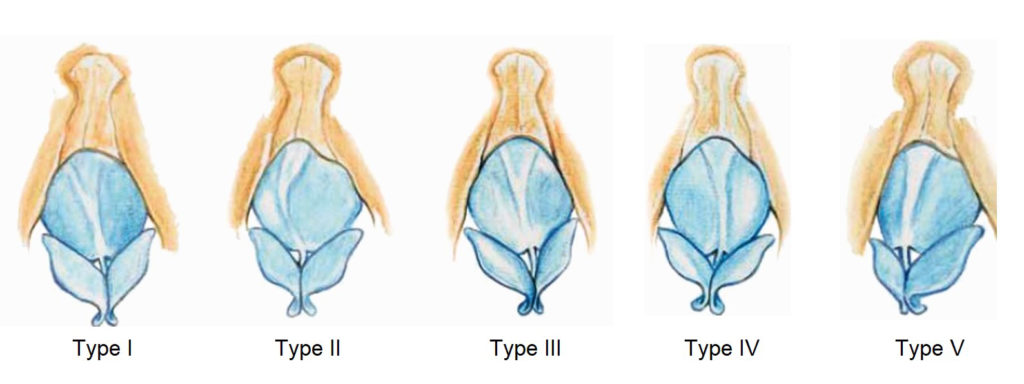
This classification system can be applied by analyzing the frontal view of the preoperative facial photograph and can be useful in establishing the preoperative treatment plan. Osteotomy can make a successful surgical outcome in cases with type 1 deviation, whereas osteotomy may not be required in cases of type 3 and 4 deviations because the axis of the nasal bone has no deviation. As type 2 and 4 deviations show severe deformation of the cartilaginous dorsum, proper treatment of the cartilaginous part is essential to acquire a successful outcome. Type 5 deviations are difficult to correct, and the appropriate correction of the deviated caudal septum is the most crucial factor for successful surgery5.
Preoperative Diagnosis And Examination
Physical examination
The surgeon must acquire the patients’ medical history before the physical examination. Careful inspection and palpation of the external nose, endoscopic examination of the nasal cavity should be performed. Acoustic rhinometry and olfactory function testing can be done to assess the function of the nose.
Facial photography
Medical photos of the patient must be taken preoperatively and postoperatively. Frontal, oblique, lateral, and basal views must be included (figure 2).
Aesthetic analysis
To analyze the deviation of the nose, the patient’s nose can be divided into three parts: upper, middle, lower thirds. These three parts should be evaluated regarding the central facial axis. The upper third consists of the bony pyramid; the middle third of the dorsal septum and the upper lateral cartilages; and the lower third of the alar cartilage, caudal septum, and alar base. As facial asymmetry is more common in patients with a deviated nose and patients with concurrent facial asymmetry often continue to perceive their nose as being deviated even after proper correction of the deviation, appropriate preoperative facial analysis is very important6.
Preoperative planning and consultation
The patient must be informed of the surgical technique, possible complications during preoperative consultation. The pisk of imperfection and recurrence also should be informed to the patient. The preoperative consultation should help the patient to set a realistic goal7.

Surgical Treatment
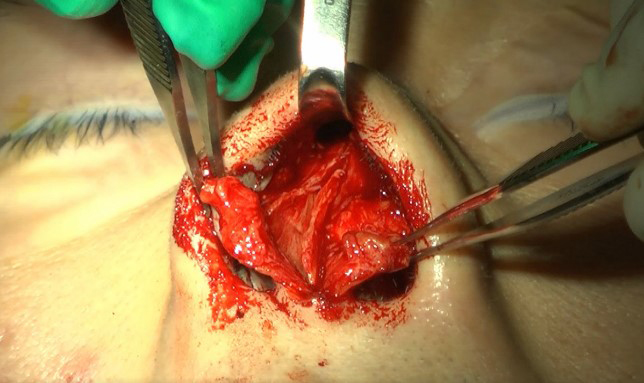
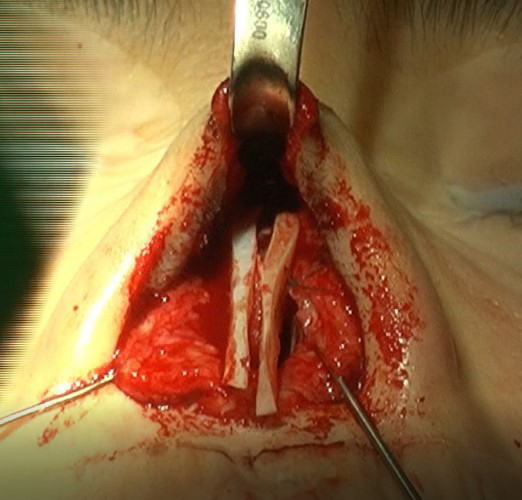
The external approach has an advantage in diagnosing anatomical problems causing the deviated nose. In addition, a more extensively exposed view can make the surgery much easier (figure 3). Risk of wound problems (hypertrophic scar, notching of the incision site, skin necrosis, pigmentation) on the incision scar presents. However, the open rhinoplasty approach should not be avoided because of the wound problems which occur in low incidence8.
Thus, the authors highly recommend using the open approach in correcting deviated noses. The surgical techniques to be described below are usually performed under the external approach.
Correction of bony pyramid
Osteotomy
It is essential to perform osteotomies properly to mobilize the nasal bone to correct the deviated bony pyramid (video 1). By performing the osteotomy, surgeons can fracture, reconstruct, and reshape the deviated bony vault into the desired form9. Instead of using conventional osteotome, an ultrasonic surgical device called “piezotome” also can be used for osteotomy and hump rasping, which can decrease postoperative morbidity and enhance healing compared with traditional instruments10.
Medial osteotomy
Medial osteotomies are used to correct a broad bony dorsum or severely deviated bony pyramid. The bony dorsum should be incised to enable the nasal bone to be separated and mobilized while maintaining the height.
Lateral osteotomy
This technique is useful when correcting the lateral outline of the bony pyramid11. As incomplete (greenstick) fracture has a high risk of recurrence of the original deviation postoperatively, complete osteotomy ensures a predictable postoperative result.
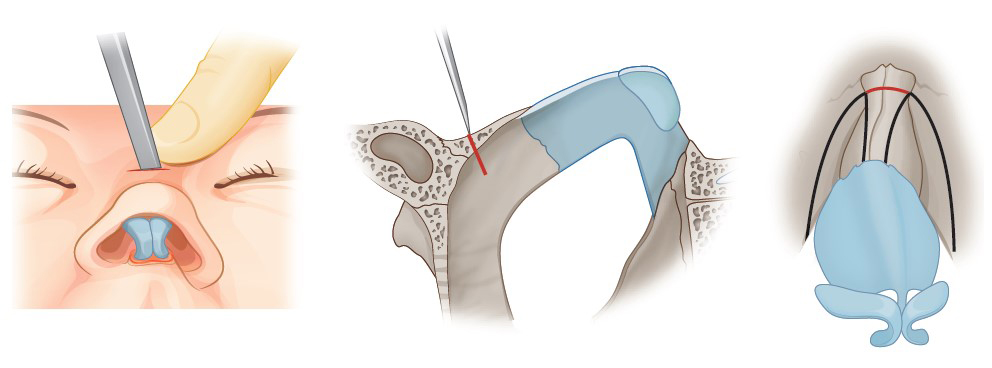
Root osteotomy
To mobilize the central bony area, root osteotomy can be a useful option12. This technique is performed by making a horizontal incision on the space between both sided of the medial osteotomy right under the nasion. It is performed at the intercanthal level, using a 2mm osteotome (figure 4). Root osteotomy must be done after the dorsal part of the cartilaginous septum is separated from the upper lateral cartilages. Risk of saddle nose deformity can be prevented by maintaining the relationship between the caudal septum and the anterior nasal spine.
Rasping
Rasping can be performed to correct partial asymmetry or protrusion after an osteotomy. It is recommended to be performed before performing an osteotomy to prevent fragmentation of the nasal bone.
Onlay grafting
Onlay grafts can be applied to the partially concave area of the nasal bone, reducing the need for osteotomies. Harvested septal bone or cartilage, fascia, or Gore-tex (W.L. Gore & Associates Inc.) can be used as grafting materials.
Correction of the septal cartilage, upper lateral cartilages, and lower lateral cartilages
The nasal septum plays a central role in maintaining the structural integrity of the nose. The correction of the deviated nasal septum via the open approach will allow the operator an excellent surgical exposure and various surgical techniques to straighten the nasal septum.
Septal cartilage correction
The authors divide the techniques for correction of deviated septal cartilage into two categories; in situ correction, extracorporeal septoplasty (Table 1).
| In situ technique | Spreader graft
Dorsal L-strut cutting and suture Caudal batten graft Caudal L-strut cutting and suture Resection of the posterior angle and reconnection to the anterior nasal spine Caudal L-strut relocation suture |
| Extracorporeal septoplasty | Extracorporeal septoplasty |
Table 1. Techniques for septal cartilage correction
In situ septal correction
Spreader graft
A spreader graft, linear cartilage graft inserted between the upper lateral cartilage and the dorsal septal cartilage is one of the most useful grafting techniques to correct the deviated dorsal septum13. It is also one of the most frequently used techniques to correct the deviated nose (figure 5). To keep the dorsal septum straight, both (concave and convex side) sided spreader grafting is highly recommended. It is best to place the spreader graft through the anterior septal angle to the gap created by the incision of the bone via medial osteotomy. If the graft is not long enough, it needs to be placed on the deviated cartilaginous area to enable the correction of deviation. It is important not to apply too thick spreader graft, which may cause mid vault widening.
The senior author usually uses extended spreader graft to obtain dorsal augmentation and tip derotation in addition to the correction of the nose simultaneously14 (figure 6).
For correction of the deviated cartilaginous dorsum, creating a new center of the lower thirds with caudal septal extension graft combined with unilaterally extended spreader graft is a useful technique (figure 7). In addition, when there is a deviated caudal septum, an extra spreader graft can be added along the caudal strut to straighten the caudal septum. Extra spreader grafts can be added if more degree of correction is needed. With this method, the direction of the dorsal strut can be changed without destructing structures of the septum.
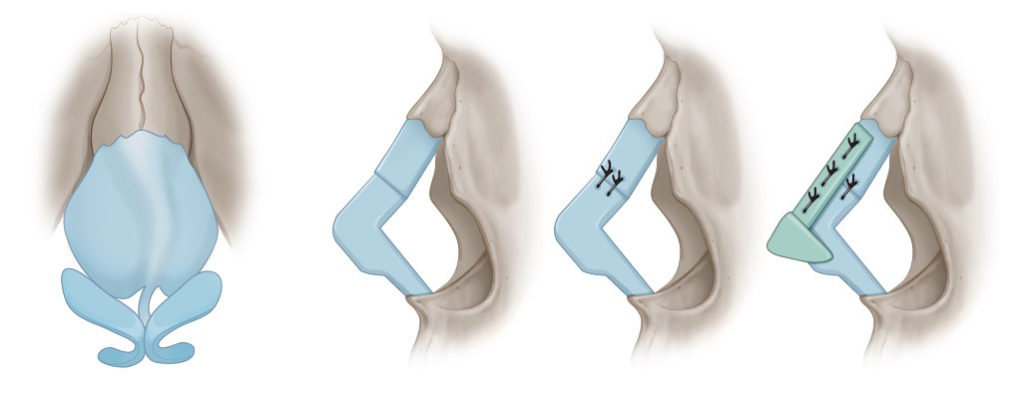
Dorsal L-strut cutting and suture technique
This technique can be applied to correct the severe cephalocaudal convexity of the dorsal L-strut. This technique preserves the keystone area and involves cutting the mid-section of the dorsal septum and reconnecting it using overlapping sutures15. This technique can shorten the length of the dorsal septum, thereby increasing the cephalic rotation of the tip. This complication can be prevented by applying an extended spreader graft of the L-strut (figure 8).
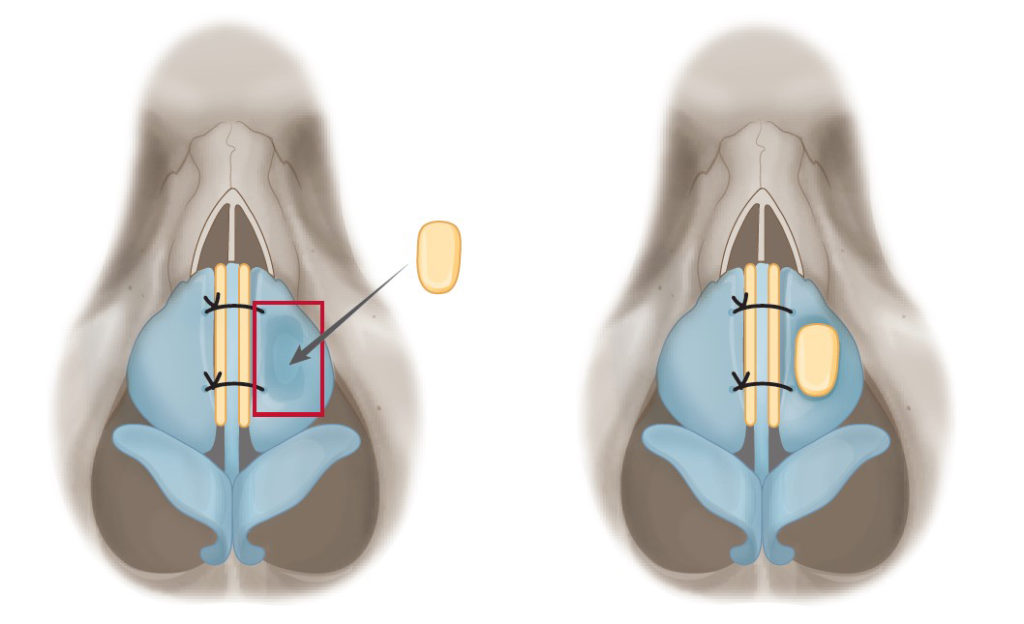
Septal batten graft
Strengthening and straightening the caudal septum is the most important step for a functionally and aesthetically successful surgery for deviated nose16. Placement of a septal batten graft made from the cartilage of the mid-part of the septum at the caudal L-strut with or without scoring incision on the concave side of the caudal septum is a very effective technique in correcting caudal septal deviation. The batten graft should be placed on the concave side, otherwise a batten graft placed on the convex side can further narrow the nasal airway. When the batten graft is extended to the anterior direction to change the shape of the tip, this is called a caudal septal extension graft. For the weak or S-shape deviated caudal septum, paired batten graft technique can be used. Placing batten grafts on both sides of the caudal strut is useful in straightening and strengthening the caudal septum. When the quantity of the harvested cartilage is not sufficient for septal batten or spreader grafting, removed septal bones also can be used for grafting17 (video 2).
Caudal L-strut cutting and suture
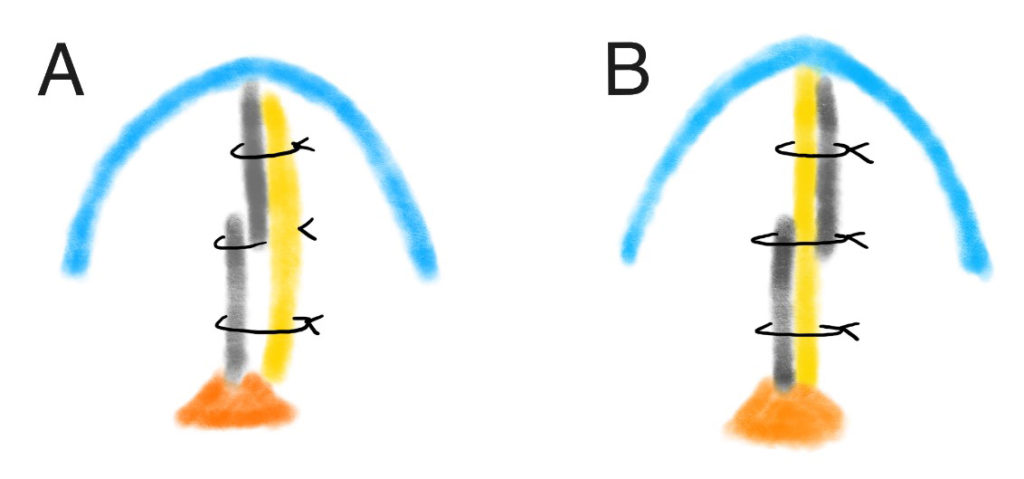
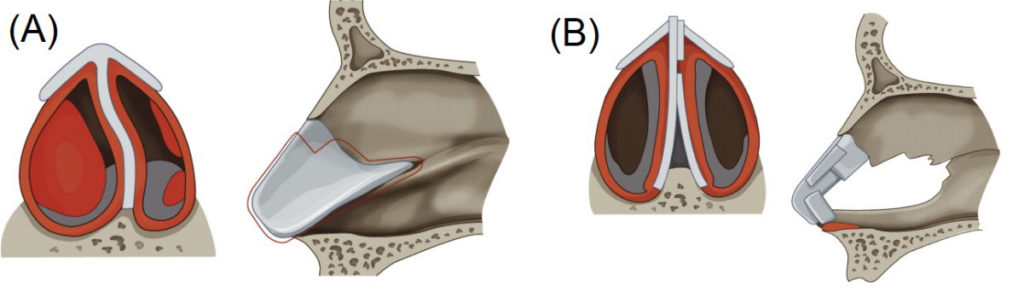
To correct C-shaped convexity or acute angulations of the caudal septum, caudal L-strut can be incised and repaired with overlapping sutures18 (video 3). When overlapping the cartilages, the surgeon must be cautious not to make the new height of the caudal septum shorter than its original height. Septal batten graft can be placed on the concave side for additional support (figure 9A).
The senior author recently introduced a novel technique called ‘caudal septal division and interposition graft’. In this technique, a batten graft is interposed between the cut ends of the caudal L-strut and sutured (figure 9B). Through this technique, the senior author could achieve successful outcomes for correcting deviated caudal septum19.
Resection of the posterior angle and reconnection to the anterior nasal spine
To straighten caudal septal deviation in anteroposterior direction, which is caused by excessive septal cartilage between the maxillary crest and the nasal roof, a small piece of septal cartilage from the junctional area between the anterior nasal spine can be removed, which will enable the caudal septum to become straight. This technique can result in saddling due to the shortening of the caudal septum. If possible, leaving enough soft tissue around the posterior septal angle and connecting it with the soft tissue around the anterior nasal spine will ensure the stability of the caudal septum.
Caudal septal relocation suture
Caudal septum needs to be separated from the anterior nasal spine and relocated to the opposite side for the linear deviation where the nose appears to be deviated to one side. If there is enough soft tissue around the anterior nasal spine, suturing will suffice for the procedure.
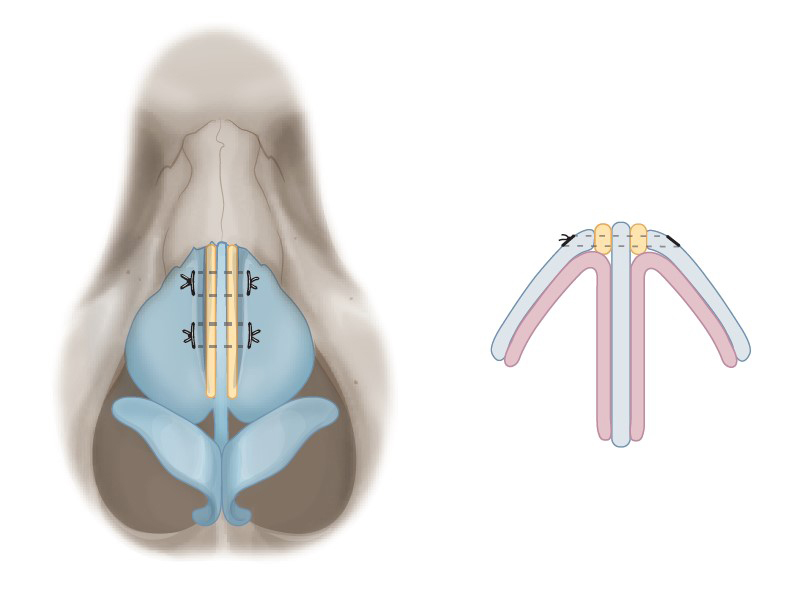
Extracorporeal septoplasty
For correction of severely deviated nasal septum that cannot be corrected with the in-situ techniques, extracorporeal septoplasty can be considered as a useful option. Compared to in situ septoplasty, better functional outcomes and comparable aesthetic results can be acquired through extracorporeal septoplasty20.
The senior author prefers to perform modified extracorporeal septoplasty technique21 (video 4). After exposing the bony and cartilaginous skeleton through the external approach, septal mucoperichondrial flaps are elevated. Then septal cartilage removal is done except few millimeters of the dorsal strip at the keystone area. With the harvested cartilage, new a L-strut is formed. The dorsal side of the reconstructed L-strut is fashioned into a Y shape by suturing a cartilage strip to the existing L-strut. The remaining cartilage at the keystone area is slotted in the fork of the arms of the Y-shaped cartilage and then sutured. The caudal septum can obtain stability by suturing the newly shaped septal cartilage to the soft tissue around the anterior nasal spine to create an inverted “Y” (figure 10).
Correction of the anterior nasal spine
If a deviation of the nasal spine presents, a greenstick fracture can be made with a gouge or an osteotome. However, complete fracture of the nasal spine must be avoided. Separating the septal cartilage and fixing it on one side of the anterior nasal spine would be a safer and easier maneuver.
Correction of the upper lateral cartilaginous deformity
As deformity of the upper lateral cartilage is usually a secondary result due to a deformed nasal dorsal septum, straightening the dorsal septum placing spreader grafts can resolve the deviation of the upper lateral cartilage. If there is remaining concavity or convexity on specific areas, insertion of an onlay graft on the concave side will correct the deformity (figure 11).
Correction of the lower lateral cartilage
When the lateral crura of the lower lateral cartilages are too big and points toward the medial direction, deformed lower third of the nose can be caused. The asymmetry or deformity of the lateral crura is responsible for the deviated nose in these patients. This can be seen in patients with the paradoxical concavity of lateral crura. With flip-flop technique (flipping the lateral crus upside down), cephalic resection, lateral crural onlay or lateral crural strut graft, these deformities can be corrected.
The deviation of the lower lateral cartilages should be first managed by correcting the nasal septum, and then be reevaluated after separating lower lateral cartilages from the upper lateral cartilages. If the lower lateral cartilages are deformed, tip surgery such as cephalic trimming, columellar strut, lateral crural overlay, interdomal suture should be performed to correct tip asymmetry.
Dorsal augmentation in deviated noses
Dorsal augmentation may be the last step in correcting deviated nose. Techniques such as osteotomies or spreader grafting which are used to correct the deviation can cause irregularities of nasal dorsum in patients with thin skin. Moreover, unpredictable complications such as the collapse of the keystone area can be occurred. For these reasons, dorsal augmentation is needed to correct the deviated nose, and the senior author recommends using soft implant materials such as Gore-tex, fascia, conchal cartilage, crushed septal cartilage, diced cartilage, and fascia wrapped diced cartilage for dorsal augmentation22. For an example, dorsal augmentation using Gore-tex is shown in video 5. Proper dorsal augmentation can prevent soft tissue deformities that cause deviation.
Prognosis And Complications
Possible complications of correction of deviated noses are incomplete correction and relapse of deviation, nasal tip deprojection due to weakened supporting structure after surgery, short nose deformity, saddle nose deformity, and incomplete correction of the nasal obstruction or newly developed nasal airway obstruction as a result of surgery.
For correcting the deviated nose, the cartilaginous and bony structures of the nose need to be opened and separated, but such an aggressive method will damage the stability of the structures over a long period of time. It can cause a recurrence of the deviation, saddle nose, short nose, and other deformities. In the senior author’s experience, the overall dissatisfaction rate in patients with deviated nose was up to 20% in his series. Especially in patients with type V deviation, the correction of linear deviation was the most dissatisfactory in surgical outcome.
References
- Tas S. The Use of Bone Dust to Correct the Open Roof Deformity in Rhinoplasty. Plast Reconstr Surg. 2018;142(3):629-638.
- Ellis DA, Gilbert RW. Analysis and correction of the crooked nose. J Otolaryngol. 1991;20(1):14-18.
- Rohrich RJ, Gunter JP, Deuber MA, Adams WP, Jr. The deviated nose: optimizing results using a simplified classification and algorithmic approach. Plast Reconstr Surg. 2002;110(6):1509-1523; discussion 1524-1505.
- Jang YJ, Wang JH, Lee BJ. Classification of the deviated nose and its treatment. Arch Otolaryngol Head Neck Surg. 2008;134(3):311-315.
- Cho GS, Jang YJ. Deviated nose correction: different outcomes according to the deviation type. Laryngoscope. 2013;123(5):1136-1142.
- Yi JS, Jang YJ. Frequency and Characteristics of Facial Asymmetry in Patients With Deviated Noses. JAMA Facial Plast Surg. 2015;17(4):265-269.
- Yu MS, Jang YJ. Preoperative computer simulation for Asian rhinoplasty patients: analysis of accuracy and patient preference. Aesthet Surg J. 2014;34(8):1162-1171.
- Kim HC, Jang YJ. Columellar Incision Scars in Asian Patients Undergoing Open Rhinoplasty. JAMA Facial Plast Surg. 2016;18(3):188-193.
- Byrd HS, Salomon J, Flood J. Correction of the crooked nose. Plast Reconstr Surg. 1998;102(6):2148-2157.
- Troedhan A. Piezotome Rhinoplasty Reduces Postsurgical Morbidity and Enhances Patient Satisfaction: A Multidisciplinary Clinical Study. J Oral Maxillofac Surg. 2016;74(8):1659.e1651-1659.e1611.
- Bracaglia R, Fortunato R, Gentileschi S. Double lateral osteotomy in aesthetic rhinoplasty. Br J Plast Surg. 2004;57(2):156-159.
- Jang YJ, Wang JH, Sinha V, Lee BJ. Percutaneous root osteotomy for correction of the deviated nose. Am J Rhinol. 2007;21(4):515-519.
- Jang YJ, Sinha V. Spreader graft in septo-rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2007;59(2):100-102.
- Lee HJ, Jang YJ. Correction of saddle and short noses. Curr Opin Otolaryngol Head Neck Surg. 2016;24(4):294-299.
- Song HM, Kim JS, Lee BJ, Jang YJ. Deviated nose cartilaginous dorsum correction using a dorsal L-strut cutting and suture technique. Laryngoscope. 2008;118(6):981-986.
- Yi JS, Jang YJ. Effect of septoplasty with a caudal septal batten graft on changes in nasal shape. Ann Otol Rhinol Laryngol. 2015;124(4):288-293.
- Jang YJ, Kim JM, Yeo NK, Yoo JH. Use of nasal septal bone to straighten deviated septal cartilage in correction of deviated nose. Ann Otol Rhinol Laryngol. 2009;118(7):488-494.
- Jang YJ, Yeo NK, Wang JH. Cutting and suture technique of the caudal septal cartilage for the management of caudal septal deviation. Arch Otolaryngol Head Neck Surg. 2009;135(12):1256-1260.
- Kim SA, Jang YJ. Caudal Septal Division and Interposition Batten Graft: A Novel Technique to Correct Caudal Septal Deviation in Septoplasty. Ann Otol Rhinol Laryngol. 2019:3489419866214.
- Lee SB, Jang YJ. Treatment outcomes of extracorporeal septoplasty compared with in situ septal correction in rhinoplasty. JAMA Facial Plast Surg. 2014;16(5):328-334.
- Jang YJ, Kwon M. Modified extracorporeal septoplasty technique in rhinoplasty for severely deviated noses. Ann Otol Rhinol Laryngol. 2010;119(5):331-335.
- Yoo SH, Jang YJ. Rib cartilage in Asian rhinoplasty: new trends. Curr Opin Otolaryngol Head Neck Surg. 2019;27(4):261-266.
Financial Disclosure: All authors have no financial interests related to the content of this article. No outside funding was received.