Abstract
Asian septorhinoplasty is a surgery procedure for reconstructing the nose with improving the air flow of the nose. Augmentation is the most commonly performed technique by increase the height of the pyramid of the nose, both dorsum and nasal tip projection. Augmentation rhinoplasty using spreader and L-shaped cartilage rib graft can improve the nasal air flow in obstructed of the nose due to the saddle or crooked Asian nose. Subjective and objective evaluation before and after procedure should be done to assess successful outcome and patients satisfaction toward surgery. Rhinoplasty Outcome Evaluation (ROE) are used to assess the level of patient satisfaction after undergoing rhinoplasty procedure. Nasal Obstruction Symptom Evaluation (NOSE), Rhinomanometry and Peak Nasal Inspiratory Flowmeter (PNIF) are methods of measurement applied in assessing airflow both subjectively and objectively.
Introduction
Facialplasty surgery has become increasingly popular over the last decade. As plastic surgeons seek to meet the increasing demand, a primary challenge is majority of patients want to maintain their ethnic identity. Any changes in the shape of the nose influence significantly to the face shape, because the nose located centrally in the face and the most prominent feature on the face.
Asians patients seeking rhinoplasty exhibit characteristics thick skin, lower radix and dorsum, smaller nasal bone, weaker cartilaginous framework, shorter columella than Caucasians, this as well the reasons of Asian nose have underprojected tip and lack in definition. The alar lobules are thick and bases are wide. Therefore, the aims surgery procedure and graft that was used are different from Caucasians. The most common
procedure in Asian are augmentation rhinoplasty to achieve higher dorsum, increase tip projection and improved tip contour.
Therefore, it is important for surgeon to do thorough history and physical examination. Several factors influence the outcome of surgery such as anatomy of the nose, operation procedure, the healing process, scar history, and characteristic of the patients (race, skin type, cartilages consistency), these must be taken into consideration for surgeon and should be inform to the patients.
Cartilage Autograft in Asian Septorhinoplasty
There are several type of grafts are used from cartilage :
Costal Cartilage Grafts
The grafts can be harvested from central portion of 6th to 8th rib cartilage, but the 7th to 8th ribs is more straighter and less warping effect. Unpredictable warping and resoption continue to be the primary problems associated with this grafts. Another disadvantages associated with donor site pain, incision scar, increased operating time, risk of pneumothorax. However when large amounts of cartilage are needed like in Asian nose, its used is indispensible. It is better to harvested from right side to prevent the posibility of confounding cardiac chest pain. Warping effect can be minimizing by carving the graft from piece of ribs to ensure adequate lenght of the graft. Carved symmetrically and concentrically from central core is another ways to reduce the risk (Figure 1). It is important to wait the early warping occurs within 15 to 60 minutes of harvesting, afterwards reshape the graft or by using diced cartilage graft to be another option for graft augmentation material.

Conchal cartilage
It can be harvested by anterior or posterior auricular incision. The cartilage grafts can be harvested from the cymba concha or cavum concha. Cavum concha can be used as tip graft because of it curved shape or can be used as dorsal graft. While, the shape of cymba concha resembles the lateral crura of lower lateral cartilage hence, it usually use in deficient or lost cases.
Septal cartilage
The most preferred cartilage in nose reconstruction, as it can be harvested from the surgical field. However it cannot be used in cases where a large amount of graft is required due to small septum in Asian nose. Kim CH, et al suggest to used posterior part of septum as a septal cartilage graft because posterior part is the thickest compared to other parts. The keystone area is important to support nasal dorum. The distance from anterior septal angle to the caudal margin of columella can be used as a reference when modelling a extended spreader graft for short nose.
Types of grafts for Asian Short Nose
Spreader Graft
Spreader grafts is a procedure in septorhinoplasty, it was proved to be helpful in functional improvement of the nasal airway. The aims of this graft is to prevent nasal valve from collapsing due to nasal obstruction. The graft are usually linear of autologous cartilage positioned between the dorsal septum and the upper lateral cartilage, they are supposed to widen the nasal valve, lengthening the nasal pyramid as well as restoration of dorsal aesthethic lines of nasal dorsum. It can also stabilized dislocated dorsal septum, maintained relationship between the septum and the lateral cartilage, straighten and lengthening the nose as well. In Asian population, this type spreader graft is very useful in reconstruction middle third crooked nose.
The spreader graft are harvested from cartilage septal graft and shape rectanguler shape, 2-3 cm long, 3-5 mm wide. This graft can be placed and extended beyond the existing caudal septum and also used to stabilized the septal extention graft. Dorsal graft form as L-shaped, was carved from rib graft and placed on top of the bony and cartilage pyramid.
Spreading graft is readily available in most primary cases, finding a long segment of cartilage to maintain the appropriate relationship between the septum and the upper lateral cartilage (Figure 2). Spreader graft can be inserted by an open and closed approach.
Spreader grafts were positioned between the upper part of septum and upper lateral cartilages after lateral and medial osteotomy.
There are 3 different methods of spreader graft. First, one extended spreader graft and one caudal septal extension graft. The extended spreader graft was sutured between the septum and upper lateral cartilage with 5-0 polydioxanone sutures. A caudal septal extension graft was placed on the contralateral caudal septum, and both grafts met as close to 90o as possible. The caudal septal extension graft was sutured with the extended spreader graft, septum, and soft tissue around the anterior nasal spine.

Second, consist of bilateral spreader grafts and bilateral batten grafts. Two spreader grafts were sutured bilaterally between the septum and upper lateral cartilage with 5-0 polydiaxone sutures. Two batten grafts were placed bilaterally on the caudal part of the L-strut and fixed with 5-0 polydiaxone sutures to the caudal septum and soft tissue around the anterior nasal spine.
Third, two extended spreader grafts and one caudal septal extension graft, used when a limited amount of septal cartilage grafts. Two spreader grafts were sutured bilaterally between the dorsal septum and upper lateral cartilage.
Study by Kim CH, et al. about cartilaginous structures of Asian Nose reported that the distance between most medial part of inferior border of the lower lateral cartilge to the alar rim was shorter in Asians than in Caucasians, and this area is called soft triangle of converse. Incision in this area can cause nasal tip deformity and notching postoperatively. The short width of this area caused marginal incision should be made with care not in order to not damage the soft tissue. They also found that the width and thickness of LLC are not adequate for cephalic resection of lateral crus.
L-Shaped Dorsal Graft
The L-shaped graft is used to augment dorsal and nasal tip. It appears that this shape are the most frequently used implants shape. This graft is used to augment the entire dorsum, especially for saddle nose cases. To reconstruct depressed of flattening nasal pyramid, rib cartilage is the most preferred for dorsal augmentation graft (Figure 3). We evaluate pre and post operative ROE, NOSE, ESS, Rhinomanometry and PNIF score in patients, and found that spreader graft and L-shaped dorsal graft (Figure 4) improved nasal breathing and has high satisfaction rate among patients.


In Asian patients, spreader and L shaped dorsal augmentation grafts can be accomplished with other graft, such as :
Septal Extension Graft
Septal extension graft is a method of controlling nasal lengthening and tip projection, rotation, and shape by fixing a graft to the septum, which lead to a strong supporting structure. This graft is taken from thick septum, ribs cartilage, and 2 layers of ear cartilages (Figure 5).
Septal extension graft may be performed in 3 different variations, extension of a spreader graft, caudal extension graft, and direct extension of the caudal septum without overlap. Caudal extension graft cause overlapping to caudal septum (Figure 6c). Byard recommends a solution for this problem which is to positioned an end to end between septal cartilage graft and caudal septum, then fixated with a vertical figure-of eight locking suture (Figure 6b), but Hyunsoo, et al. suggest a variation of vertical figure-of eight locking suture that firmer and tighter than Byard (Figure 6a). The variety of shape to achieve specify goal tip contour.


Multilayer tip graft

This graft positioned to elevate the nasal tip for better definition. It is a fusion between 2 or more autografts such as septal or conchal cartilage. This spesific graft is useful to make nasal tip more prominent and better definition in Asian nose (Figure 7).
Approach in Asian Septorhinoplasty
Endonasal Approach
In Asian rhinoplasty, deviated and/or short nose can be corrected with spreader grafts using endonasal approach instead of open approach. The nasal skin and the underlying soft tissue are undermine in order to distinctly expose the septal and upper lateral cartilages. Upper lateral cartilages are separated from the septal cartilages. Next, the harvested cartilages are positioned between the upper lateral cartilage and the upper part of septal cartilage on both sides.
Hemitransfixion Incision for Approaching Nasal Septum
Cottle clamp and alar protector are used to expose the caudal septum and identified the caudal end septum. Left hemitransfixion incision is used as opening incision, start from 1-2 mm behind caudal end septum to the anterior of nasal spine and parallel to the caudal end of septum using blade No.15 (Figure 8a). Elevation of the mucoperiosteum from the left side of the septum, anterior, posterior and inferior tunnel. Placement nasal speculum inside through hemitransfixion incision to the left anterior tunnel. Then used cottle elevator to continue elevate mucoperichondrial and mucoperiosteal to the perpendicular plate ethmoid anterior of sphenoid (Figure 8b).

Care is taken to prevent mucosal tears by widen incision and flap. Elevate submucoperichondrial flap and separate the bony cartilage junction using the respatorium. Metzenbaum suggest a procedure called “swinging door” by disarticulated intercartilaginous from nasal margin, maxillary crest groove, and bony septum using cottle elevator and leaving only its superior attachment .Then use cottle knife to incise the cartilage and remove any deviation. 1 cm from caudal end septum should be preserve for anterior and dorsal L-strut for nasal tip support.
Caudal septal deviation in lower third nose is the most common reason for septoplasty. The asymmetry of lower lateral cartilage should be mobilized by releasing scar tissue and continue with graft augmentation. The correction of these defects are challenging procedure because simply resecting the caudal segment cause losing tip support and shortening of the columella. The caudal deviation can be corrected by extending the spreader grafts to the anterior septal angle. Yong et al, introduce the cutting and suture technique of the caudal L-strut for septal deviation by excise the deviated septum at the most curved region in the caudocephalic direction, and put the upper and lower strut overlapped and sutured it together in the midline.
Intercartilaginous Incision (Eversion/Retrograde technique) and with marginal incision (luxation technique) for Approaching Nasal Dorsal and Nasal Tip .
Eversion (retrograde) technique start with intercartilaginous incision by putting retractor in alae and use ring finger to press alae and expose the vestibulum and valve area (Figure 9).
Luxation technique usually start with marginal incision, which is made laterally to medially on subcutis along caudal crus lateral, dome, and anterior part of medial crus of cartilage alae to expose the inferior of lateral crus (Figure 10a,b).


Open Approach
A transverse inverted V incision is made on one third from the base of collumella using blade No.15, followed by bilateral infracartilaginous incision (Figure a, b). The nasal tip skin gently dissect through infracartilaginous incision from the caudal margin middle crura with pointed, slightly curved scissors and continue to dissect and elevate the skin from middle crura with angulated scissors (Figure 11c). The skin and the soft tissue is taken upward using two-pronged hooked, gently dissection and prevent laceration that cause postoperative retraction and scar (Figure 11d). Dissect laterally to lateral alae crus cartilage, upper lateral cartilage, dorsum nasi, until naso-fronto angle and caudal end septum is exposed with curved scissor.
Spreader graft was inserted between the upper lateral cartilage and septum, continue with fixation using PDS suture or prolene 5-0. Septal extension graft was sutured end to end septum or overlapped with the caudal end septum depend on graft design. L crus dorsal graft was inserted into interdormal area between dome and intermediate crus lower lateral cartilage. Incision was closed with a monofilament 5-0 or 6-0 suture.

Case 1
A female patient, with crooked nose type 2 and severe deviated septum type 6 due to traumatized nose (Figure 12a, b). The patient underwent open septorhinoplasty with structural graft, the surgery start with V inverse incision continue with undermining and spreading to the lower lateral cartilage to approach caudal end septum and underwent septal correction. The paramedial, lateral, transverse osteotomy were perform (Figure 13). The bilateral spreader graft were inserted between upper lateral cartilage followed by putting L-shaped dorsal rib graft beneath of it (Figure 14a). The multilayer tip graft was inserted for better nasal tip defining point (Figure 14b). The result after the surgery, straight nasal dorsal browtip aesthetic line and improve tip defining point (Figure 12c, d).


Case 2.
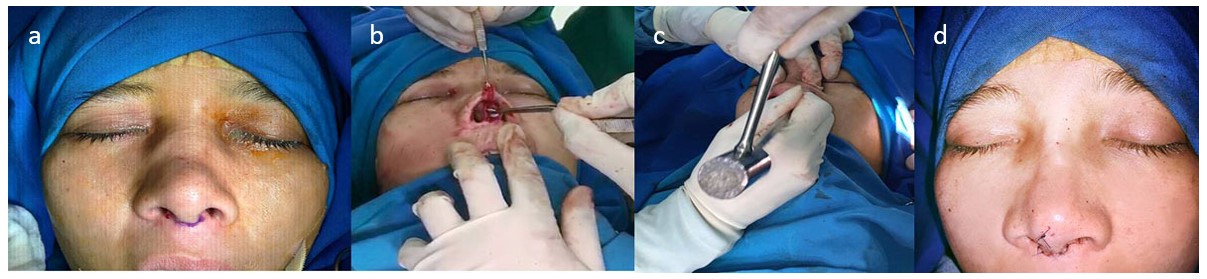
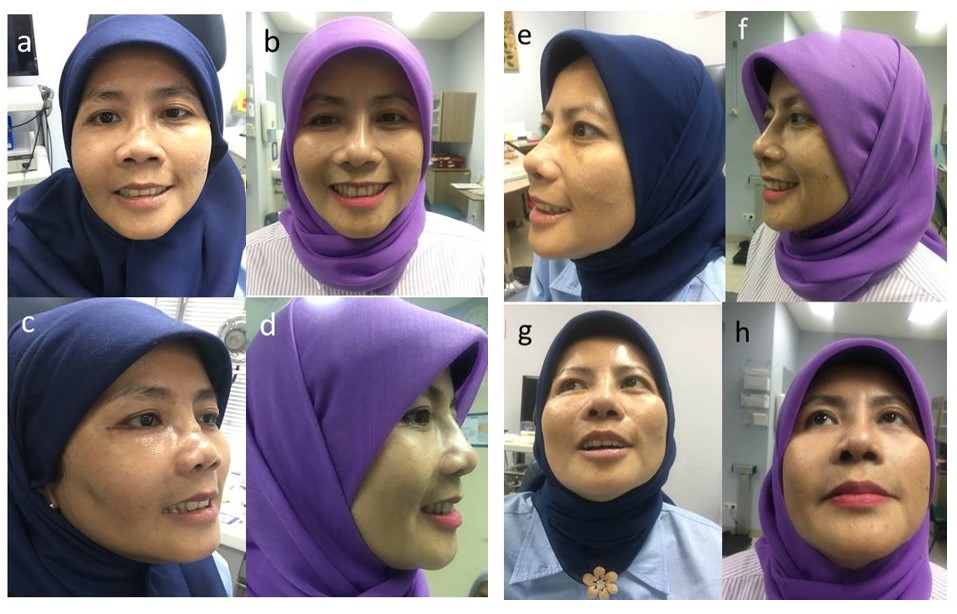
A female patient, came with nasal obstruction and diagnosed as severe saddle nose (Figure 15 a,c,e). The patient underwent augmentation septorhinoplasty with open approach technique (Figure 16c). The bilateral spreader and L-shaped dorsal augmentation graft were inserted to the right position combine with septal extension and finally cover with shield graft (Figure 16a).
Shield graft can increase tip more projecting and as septal extension graft can provide structural support. Another advantage of this graft is it make the tip looks natural and pointed nasal tip.
The postoperative result showed straight nasal, browtip aesthetic line, increase nasal tip (Figure 15 b,d,f).


Case 3
A female patient with severe saddle nose and short nose due to trauma, underwent spreader and L-shaped septorhinoplasty (Figure 17). A short nose is one of the most difficult deformities to correct, and it requires the use of multitude of challenging surgical technique for adequate correction.
Successful correction of this deformity can be obtained by extending the internal framework of the nose and the external soft tissue envelope. In lengthening the nasal skeleton, an extended spreader graft using costal cartilage, multilayer tip grafting, and lateral crural strut grafting are important technique.
The patient nose is accompanied by over rotation of the tip and saddle nose as well. The septal extension graft in combination with extended spreader graft, is effective for lengthening her short noses, counterrotating the nasal tip and maintain nasolabial angle. Sufficient lengthening of the patient nose can be more easily achieved by using a strong extended spreader graft made from costal cartilage. It is placed on both sides of septum at a position that is 3 to 10 mm more caudal than the anterior septal angle. When the remaining L-strut is thin and weak, the dorsal and caudal struts should be reinforced by strong and thick costal cartilage. These various form of grafts are stabilized nasal base to maintain the desired tip contour, position and resist the contractile forces of healing.
References
- Blanco M, et al. Functional and aesthetic result after augmentation rhinoplasty. Hospital Universitario A coruna. Spain: A Coruna, 2011; 62(5):347-354.
- Tardy M. Nasal Reconstruction and Rhinoplasty. In: Snow J, Ballenger J, editors. Ballenger’s Otorhinolaryngology Head and Neck Surgery. 16th editi. Spain: BC Decker; 2003. p. 842–99.
- Ishii CH. Current update in asian rhinoplasty. Plast Reconstr Surg Glob Open. 2014;2(4):e133.
- Jin HR, Won TB. Recent advances in Asian rhinoplasty. Auris Nasus Larynx. 2011; 38(2): 157-164.
- Moretti A, Sciuto S. Rib grafts in septorhinoplasty. Acta Otorhinolaryngol Ital. 2013;33(3):190–195.
- Nataraj RV, Mohan J, Reshma, et al. Augmentation grafts in septorhinoplasty : our experience. International Journal of Otolaryngology and Head & Neck Surgery. 2015;4 :317-324.
- Kim CH, Jung DH, Park MN, Yoon JH. Surgical Anatomy of Cartilaginous Structures of the Asian Nose: Clinical Implications in Rhinoplasty. The Laryngoscope. 2010;120(5):914-9.
- Teymoortash A, Fasunla JA, Sazgar AA. The value of spreader grafts in rhinoplasty: a critical review. Eur Arch Otorhinolaryngol. 2012;269(5):1411–1416.
- Kim H, Han K. Asian Rhinoplasty: Correction of the Short Nose with a Septal Integration Graft. Semin Plast Surg. 2015;29(4):269–277.
- Reh DD, Kasperbauer JL, Facer GW, et al. Reconstructive surgery of the nasal septum. Facial plastic and reconstructive surgery,4th edition. New York :Thieme;2016.p.553-566
- Jang YJ, Yeo N, Wang JH. Cutting and Suture Technique of the Caudal Septal Cartilage for the Management of Caudal Septal Deviation.Arch Otolaryngol Head Neck Surg.2009;135(12):1256–1260.
Acknowledgement: the author acknowledge Dewo Affandi, MD,ORL-HNS for contributing photos, Sigit Sutjipto and Widi Sutjipto as illustrator, Gracelia Christiani as writer draft.