Abstract
Latino patients are also known as hispanic or mestizo and are a combination of different ethnic groups that originate from Spanish speaking countries from around the world. When performing surgery on this group of ethnic patients, the goals are to achieve a natural looking appearance preserving patient’s ethnic features and hopefully fulfilling the patients’ desires. A gradual approach to the nose is presented where support structures are reinforced; techniques are used to increase rotation and definition without necessarily making the nose look bigger. A judicious selection of suturing techniques and placement of grafts is presented. The final surgical result should be a nose that blends in with the patients face without looking operated or overdone.
Introduction
Civilizations over time have always had a genuine interest in beauty and ethnic groups around the world are not the exception. Migration patterns of different ethnic populations looking for better working opportunities and improvement in their quality of life have changed the racial composition in many countries and regions. Today pure races tend to be less prevalent and facial plastic surgeons worldwide are faced with patients of many different cultural and ethnic groups wanting to improve their looks.
The most important migrations from Latin American countries have been to United States and Spain and to a lesser degree to other European countries and to Canada. Most of the population have established themselves in these new countries and with time have become part of the society that has received them.
Definition of Latino
Latino can be defined as “a person of Latin-American origin living in the United States. 1 Latino is a term that in the United States can often be used interchangeably with hispanic or mestizo without any offense meant. It refers to people coming from Spanish speaking countries mainly Latin American countries. The terms latino and hispanic are related to where the person is coming from. In United States the terms are used interchangeably and refer mainly to people coming from Mexico, Central and South American countries.
Mestizo is a term used to define racial features. It is defined as a mixture of races mainly Indian, Caucasian and Negro. The predominant features will vary depending on where the patient comes from and what specific migration patterns have occurred in that geographical area. A strong influence of Caucasian features (European countries) can be found in patients coming from countries like Argentina and Chile. Indian features are predominant in countries like Perú, Bolivia, Mexico, Guatemala and other Central American Countries. A stronger African influence is seen in countries like the Caribbean Islands, Cuba, Brazil, and the coasts of Venezuela and Colombia. In spite of all this, mestizos are defined as being a mixture of racial features.2-5 It will be the surgeon’s responsibility to adequately define the patients characteristics and underlying anatomical problems.
Anatomical Characteristics of the Latino, Hispanic or Mestizo Nose
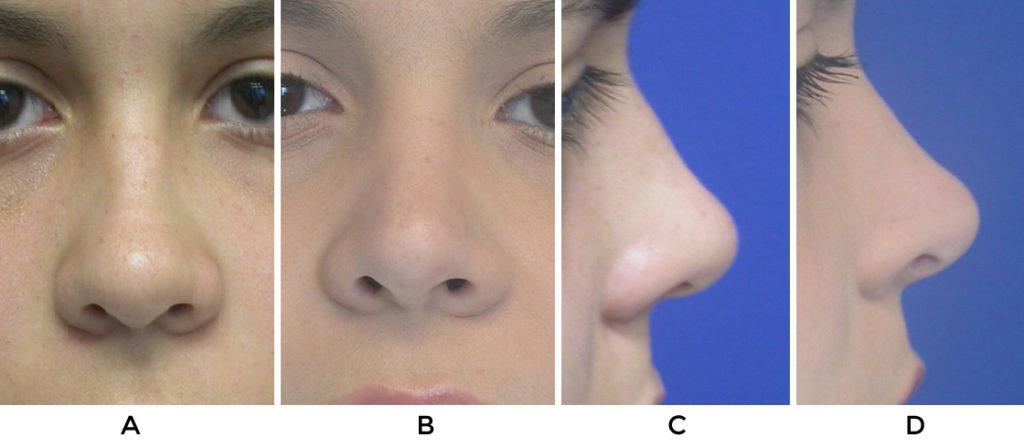
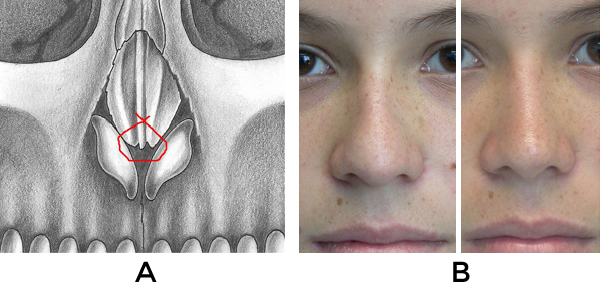
As we mentioned before, mestizo is defined as a mixture of racial features. Anthropologically, three big groups are used to define nasal features: platyrrhine, mesorrhine and leptorrhine.6,7 The platyrrhine nose is usually flat and wide and is usually seen in patients with predominant negroid racial features. The leptorrhine nose tends to be tall and narrow and is more related with Caucasian or northern European patients. The mesorrhine nose is that seen in the mestizos of Latin America and is considered an “in between” stage between the platyrrhine and the leptorrhine nose. Characteristics in these patients tend to be more modest than those found in leptorrhine noses. The underlying bony and cartilaginous support structures of the nose tend to be weak. Nasal bones have a tendency to be small and slightly wide although it is not uncommon to find a deep radix accompanied by a small dorsal hump.
Tip support mechanisms tend to be deficient. The nasolabial angle tends to be more acute, the nasal spine is smaller, the columella can be shorter and the shape of the nostrils will be more rounded or horizontal looking.
Alar cartilages although wide, tend to be weak and flimsy resulting resulting in poor projection and rotation of the nasal tip.5 (Table 1, Figure 1)
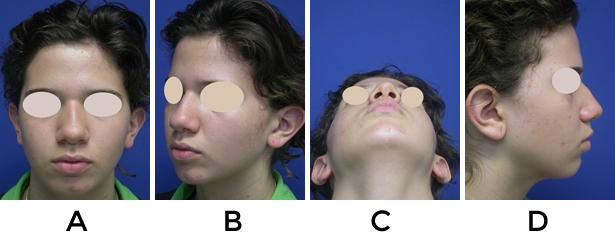
Table 1. Nasal Characteristics of Mestizo Patients
| NASAL CHARACTERISTICS | MESTIZO PATIENTS |
| Skin Type | Normal/ Thick/ Sebaceous |
| S-STE | Thick/ tendency towards inflammation |
| Nasal Bones | Small |
| Bony Dorsum | Normal to low radix Wide nasal bridge |
| Cartilaginous Nasal Vault | Normal to Weak , wide |
| Nasal Tip/ Alar cartilages | Flimsy/ unsupportive/ wide/ undefined |
| Columella | Normal to short |
| Nasolabial angle | Normal to acute |
| Nasal spine | Normal to short |
| Tip Recoil | poor |
| Nostril shape | Horizontal shape |
| Alar Base | Normal to wide |
Preoperative Evaluation
a. Consultation
Having the time and being able to communicate with the patient in an adequate manner is fundamental if the surgeon wants to establish an appropriate relationship with the patient. Several issues must be covered during the consultation:
- Define the patients ethnic, racial and cultural background.
- Define the patient’s desires and expectations. Does he/she want to preserve ethnic features or is there a clear desire for a more dramatic change in appearance.
- Complete previous medical history including previous surgical and non-surgical procedures on the nose and face including procedures performed by aestheticicians.
b. Physical Examination
1.Functional Evaluation
The function of the nose should be evaluated with an internal and an external examination. This is done using a headlight, palpating external structures and progressing to an internal exam with a nasal speculum and if indicated a flexible or rigid nasal endoscopy.
The following aspects should be properly documented:
a. alar collapse.
b.evaluation and/or compromise of internal or external nasal valve.
c. septal deviations/ availability of septal cartilage for harvesting.
d. turbinate hypertrophy.
e. sinus disease.
2.Aesthetic Evaluation
- Facial characteristics/ presence of facial asymmetries/ deformities/ scars
- Definition of skin type/ thickness of S-STE
- Definition of nasal characteristics
- Upper Third of Nose: Bony dorsum
- Middle Third of Nose: cartilaginous dorsum
- Lower third of nose: nasal tip
C. Photography
A set of standard rhinoplasty photographs should be obtained. These should include: frontal view, base view, Lateral views (left and right), left and right oblique views. The author routinely uses computer imaging to show possible surgical changes and evaluate before and after images. This helps the patient evaluate if those are the surgical changes he wishes to have and understand the limitations of the surgical procedure. When using computer imaging, the expertise of the surgeon becomes crucial in defining how much of a realistic change will be obtained. This will help surgeon define what surgical options can be offered and will help the patient understand the extent of the procedure that is going to be performed.
Photography automatically becomes part of the medical record and is useful not only during the consultation with the patient. The author uses printed copies of the pictures during surgery and the pre-surgical images are constantly used to evaluate the patients’ evolution during follow-up visits after surgery. Post-surgical pictures should be taken ideally at 6 months and 12 months after surgery. This helps evaluate aesthetic outcomes, surgical techniques and becomes a valuable tool when performing long term follow up on patients.
D. Discussion and Explanation of possible surgical options
Step-Wise Approach to the Latino or Mestizo Nose
The latino or Hispanic population comprises a big heterogeneous group. Anatomical findings will really depend on which racial features are predominant. The big question we have to ask ourselves as surgeons is: “what do our patients want?” In general mestizo patients want smaller noses that look more defined. A step-wise approach is necessary to be able to establish an accurate anatomical diagnosis, define what problems the patient has, what are the problems the patient wants corrected and what are the possible surgical solutions.

Anatomical Diagnosis
Definition of existing problems
Definition of what problems the patient wants to correct
Definition of surgical approaches and techniques
Problem-wise most of our patients tend to have a thick S-STE and a weak underlying structural framework (bony and cartilaginous). The surgical techniques used should all be oriented towards preservation and strengthening support structures of the nose, conservative tissue excision and use of sutures and grafts to help define the different anatomic structures of the nose 8,9.
Surgical Techniques
All cases are performed under general anesthesia and the external approach is used in most patients. The functional aspects of the nose are addressed first before doing any cosmetic procedures. Standard endoscopic sinus procedures can easily be performed without any postsurgical complications. In patients with turbinate hypertrophy, these are routinely treated with endoscopic turbinoplasty procedures. Septal deviations are corrected and cartilage is harvested for grafting. The amount of quadrangular cartilage present in mestizo patients is not very big and like in most mesorrhine patients it usually is not thicker than 2-3mm.10,11
There is no “standard” surgical technique for latino or mestizo patients. Several general “rules” should be followed to ensure predictable long term results: 1. Support structures of the nose should be preserved or strengthened 2. Conservative tissue excision 3. Structural grafting to improve nasal tip support 4.Use of sutures or grafts to help define the nasal tip. 8,9 With this philosophy in mind, the surgeon must choose how and where he is going to use his grafting material in a wise manner. The amount of septal cartilage that is available can be insufficient for all the possible grafts that could be used in some of these patients. If an organized surgical plan has been defined, choices can be made more easily and mistakes which will translate into unsatisfactory results can be avoided.
Problem-wise and to help plan surgery in a proper fashion, the nose can be divided into thirds:
-UPPER THIRD OF THE NOSE (BONY DORSUM)
-MIDDLE THIRD OF THE NOSE (CARTILAGINOUS DORSUM)
-LOWER THIRD OF THE NOSE (NASL TIP)
The bony and cartilaginous dorsum is managed before any nasal tip procedures are performed.
Upper Third of the Nose (Bony Dorsum)
The nasal bones of our patients tend to be short. Even though humps can be found in some of our patients, it is more common to have dorsums that tend to be low and wide
Common Anatomical Findings:
- wide dorsum without hump and normal radix
- low radix with bony dorsal hump
- low nasal dorsum
Surgical solutions:
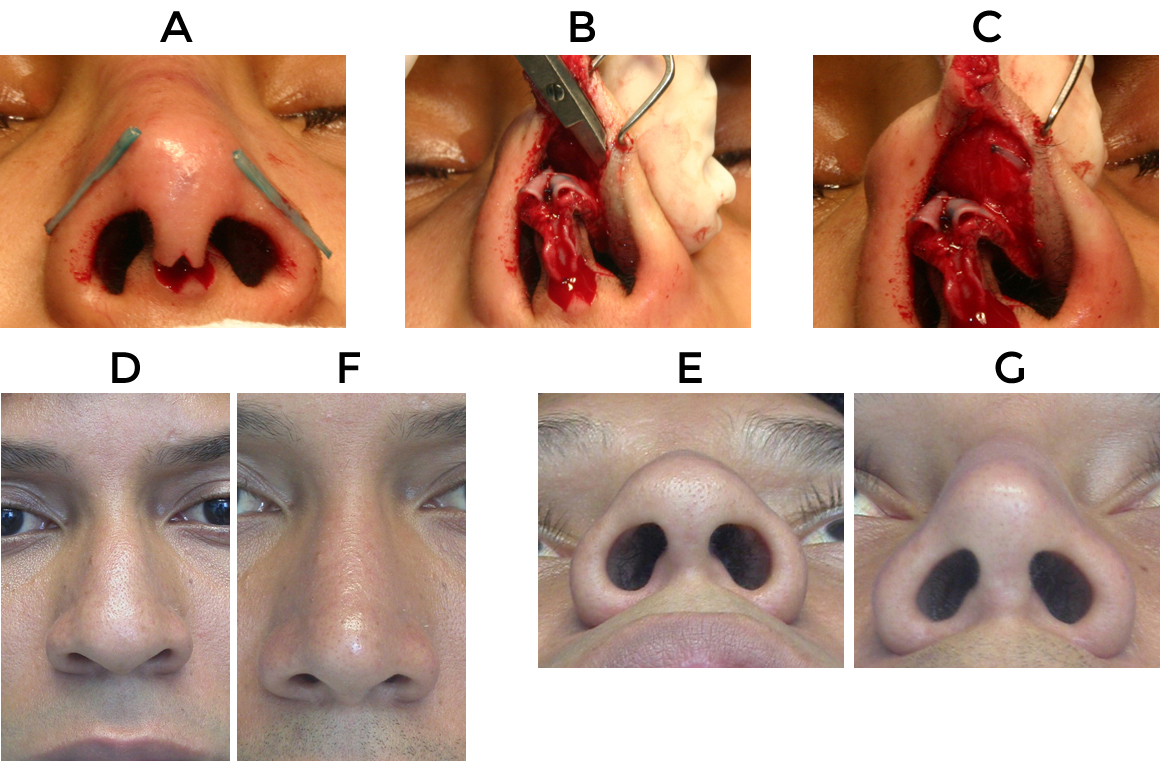
Medial and lateral ostoeomies: will help narrow a wide bony dorsum. Medial osteotomies are done in a curved fashion before the lateral osteotomies using a 3mm osteotome. It is important to curve osteotomes 15-20 degress off the midline to avoid going all the way up to the nasofrontal bone. Lateral ostetomies are performed in a high-low-high fashion using a 2.2 guarded osteotome. Medial osteotomies are performed when there is a wide dorsum without a hump or a crooked nose. Lateral osteotomies are performed in most cases. In the cases where there is a very wide bulbous tip with thick skin, and a straight dorsum, no osteotomies are performed. (figure 2)
Bony dorsal humps: can be reduced either with an osteotome in a very conservative fashion or with graded rasps. The cartilaginous portion of the hump is removed with a #15 blade taking out thin slivers of cartilage until the desired height is obtained. It is not infrequent to have to remove portions of the septum (dorsal portion) and the upper lateral cartilages. If possible the nasal mucosa should not be disrupted. This will help prevent secondary collapse of the upper lateral cartilages.

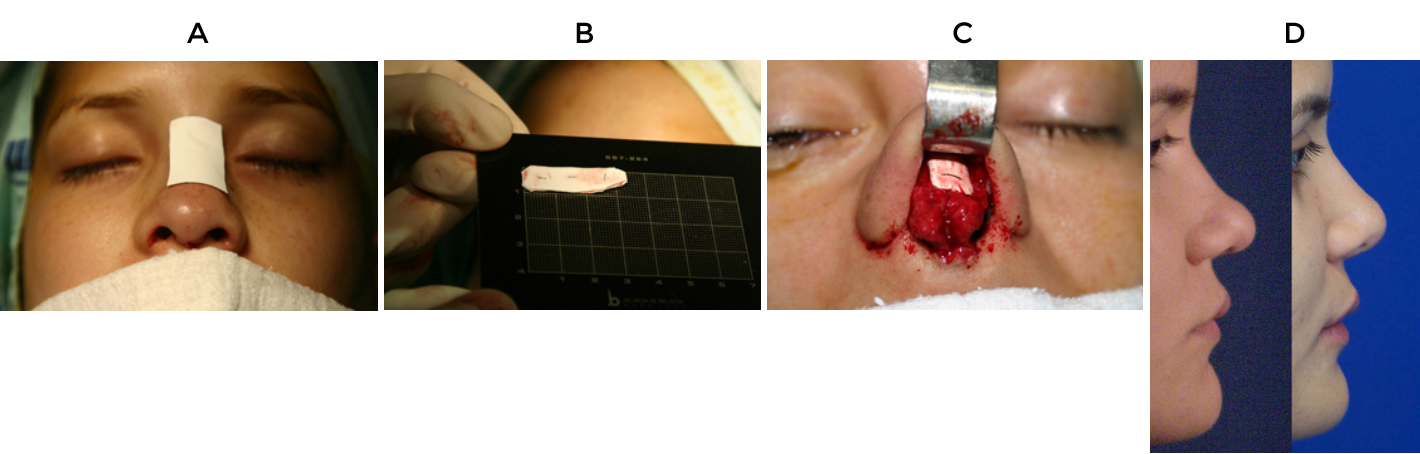
Radix graft: in those cases where there is a low shallow radix with a small dorsal convexity and short nasal bones, a radix graft can be placed using morcelized cartilage to fill in this space and avoid lowering the convexity of the dorsum. This helps build up the dorsum without making the nose look much bigger and is an excellent alternative to the use of implants on the nasal dorsum. 9,12
Radix graft+ lowering of bony dorsal hump: Frequently a combination of both techniques can be used. Crushed cartilage is placed as a radix graft and only conservative rasping of the dorsum is performed. In this fashion height of the dorsum is preserved (Figure 3).
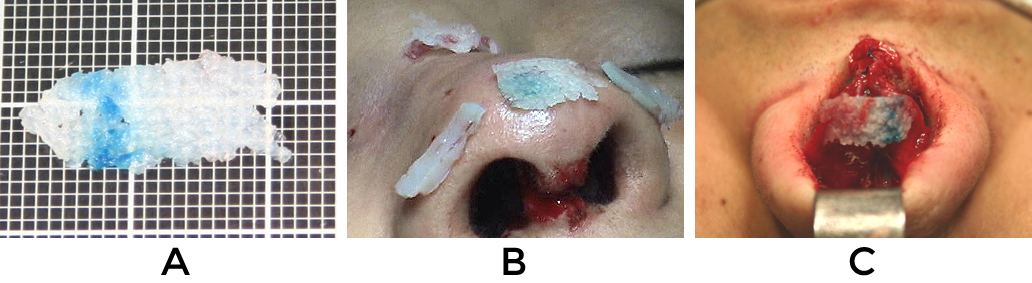
Dorsal augmentation: Ideally should be performed with cartilage and in the author´s experience, septal cartilage is preferred over auricular cartilage. All edges should be well trimmed and beveled so they won´t be noticeable over time. If more dorsal augmentation is needed, alloplastic material like expanded polytetrafluoroethylene (Gore-Tex) sheeting can be used with a low complication rate. Material should ideally be placed in precise pockets and if possible fixed with sutures to the middle third of the nose to avoid shifting. (figure 4).13,14
Middle Third of the Nose
Latino patients tend to have weak support structures in the nose. It is not uncommon to find patients with short nasal bones and weak upper lateral cartilages that have a tendency to collapse. Any dorsal work performed on the nose will tend to increase this inherent weakness especially if humps are going to be reduced or medial osteotomies are going to be performed. Preventive measures like structural grafting with spreader grafts or placement of reinforcement sutures in the middle third of the nose can help avoid postsurgical complications like inverted v deformities of the upper lateral cartilages (ULC), collapse of any of the lateral cartilaginous sidewalls of the nose or compromise of the internal nasal valve.
Anatomical Findings:
- Weak upper lateral cartilages
- Flattened / wide middle third of nose
Surgical Solutions:
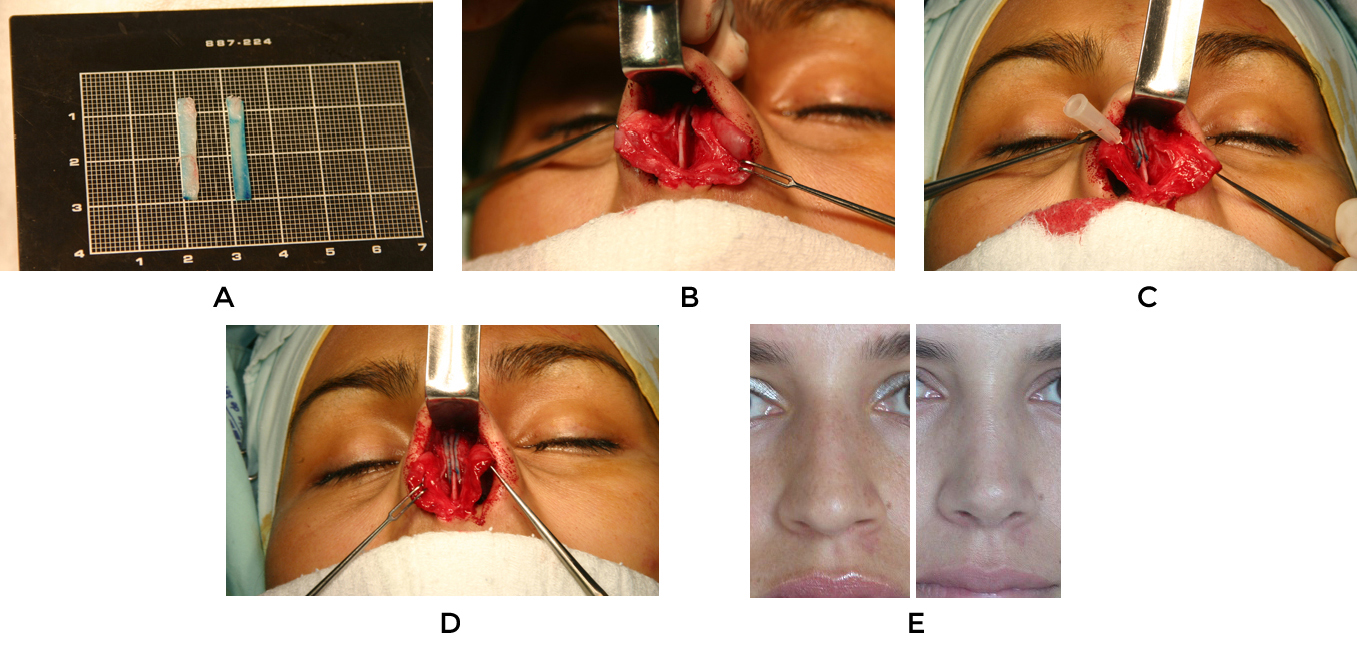
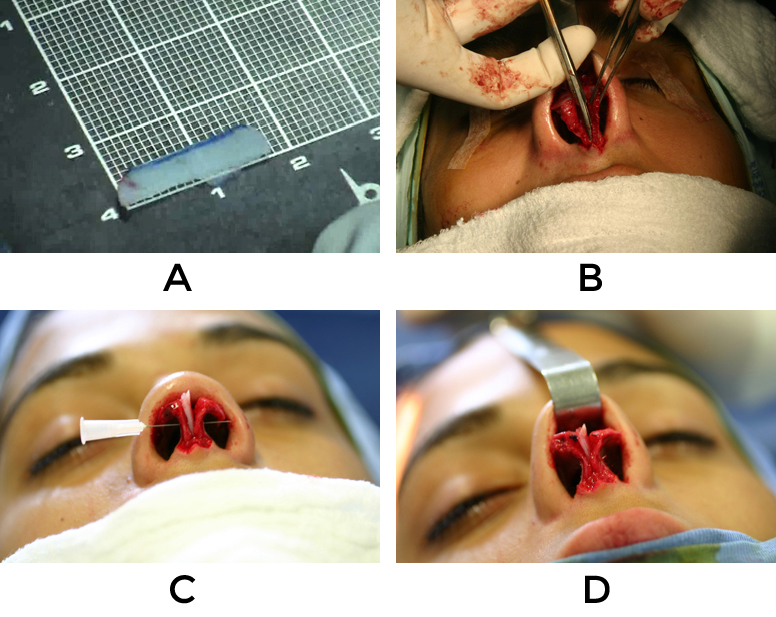
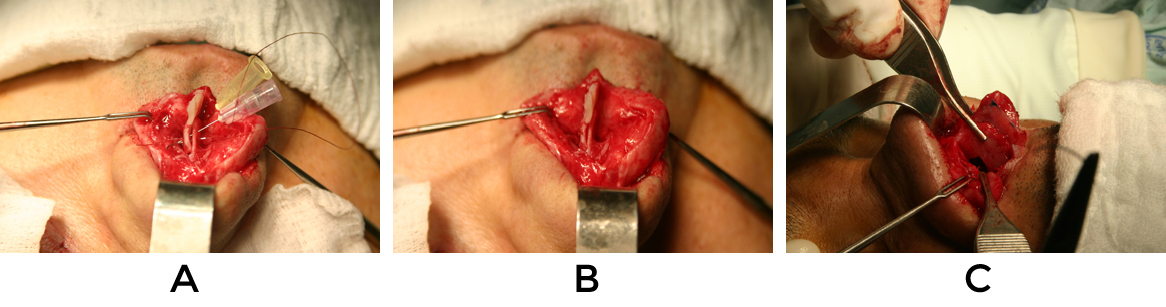
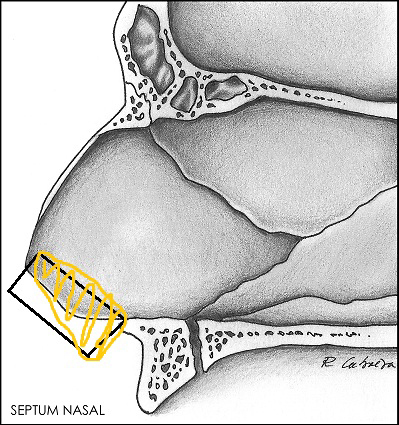
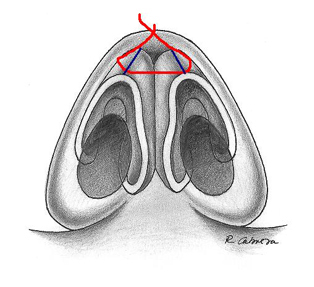
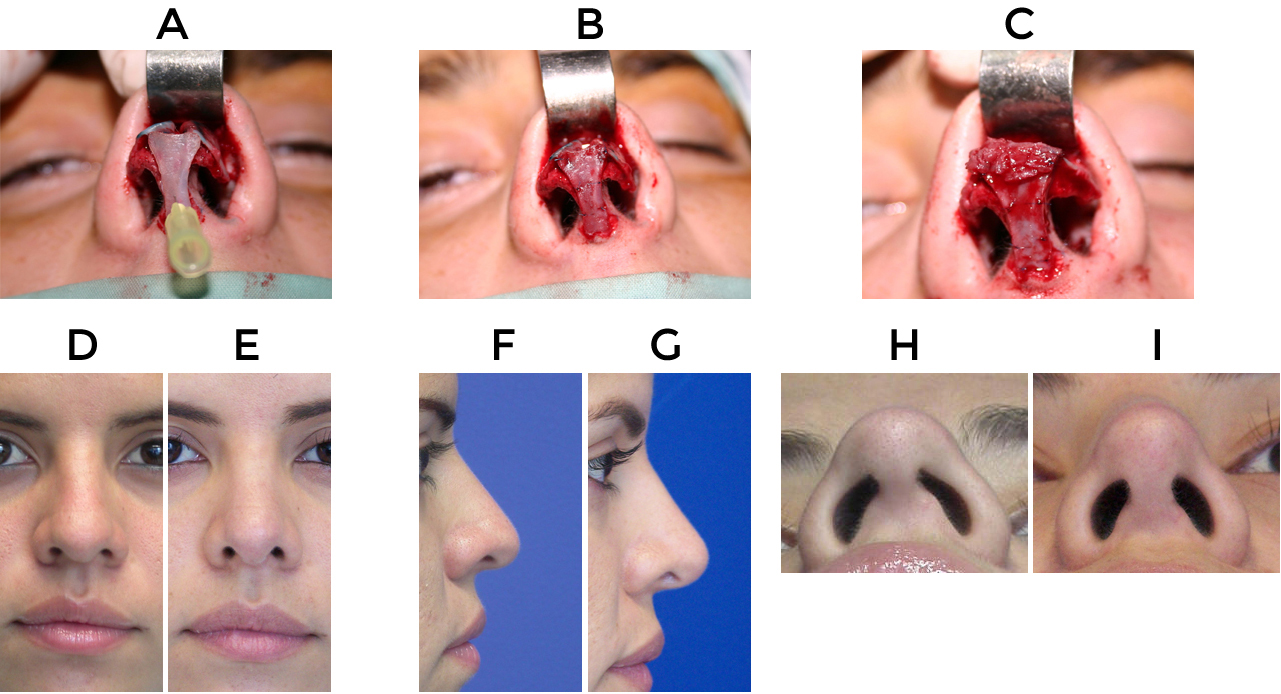
Spreader grafts: are rectangular pieces of cartilage that are carved from the nasal septum, auricular concha, and in special cases from rib cartilage. The thickness of the graft will be given by the type of graft that´s used but with the exception of rib the dimensions will vary between 1-3mm. The height should not be more that 3-5mm and the length can be 15-20mm depending on the individual patient´s needs.
Spreader grafts are used to give additional structural support to the middle third of the nose when any dorsal work has been performed, or to strengthen the middle third area in the cases where there is a natural weakness or collapse of any of the upper lateral cartilages.15 These grafts help maintain the anatomical trapezoidal contour preventing the postsurgical appearance of an inverted “v” deformity. If there is a previous crooked nose with any dorsal septal deviations, uni or bilateral spreader grafts will help in this correction. The length of the grafts is tailored according to patients needs. They can extend from the nasal bones all the way down to the caudal edge of the septum or can be circumscribed in one small area of the middle third of the nose (figure 5). It is important that the grafts are not too wide because this could produce nasal obstruction especially at the nasal valve area.
Sutures: Mattress sutures using 4-0 or 5-0 absorbable material can help align the upper lateral cartilages to the dorsal edge of the nasal septum and are always used by the author if any conservative resection of the cartilaginous dorsum has been performed to securely position the upper lateral cartilages to the dorsal edge of the nasal septum.
Onlay Grafts: can be used to help camouflage persistent depressions over the upper lateral cartilages. Morcelized cartilage can also be used to smooth out or fill in defects.
Lower Nasal Third of the Nose
From a practical standpoint, the nasal tip can be divided in two big areas: the pedestal and the tripod. The pedestal is a more rigid structure that is formed by the caudal end of the septum. The tripod is more flexible and is formed by the conjoined medial crura and both lateral crura and sits on top of the pedestal. These structures, as mentioned earlier are covered by the S-STE giving the final shape to the nasal tip. The nasal pedestal is addressed before any final tip work is done. In this way projection and rotation will not be lost after tip remodeling techniques are performed.
The lower third of the nose is also referred to as the nasal tip. It can be divided into two areas: the nasal base and the nasal tip. The nasal base or pedestal is a more rigid structure that is formed by the caudal end of the septum and the nasal spine. The tripod is formed by the conjoined medial crura and both lateral crura. It is more flexible and sits on top of the pedestal. 16,17
Latino patients tend to have bulbous tips that sit on bases with poor support. Any work that is performed on the tip first requires a stable nasal base in order to be able to modify structures and place grafts. The techniques that are used more frequently are the columellar strut or the septal extension graft. 9
Anatomical Findings:
- A caudal septum that tends to be short and weak resulting in an acute nasolabial angle
- Short columella
- horizontally shaped nostrils that are the result of a weak tripod and pedestal structure
- disproportion in the ala/columella relationship
Surgical Options:
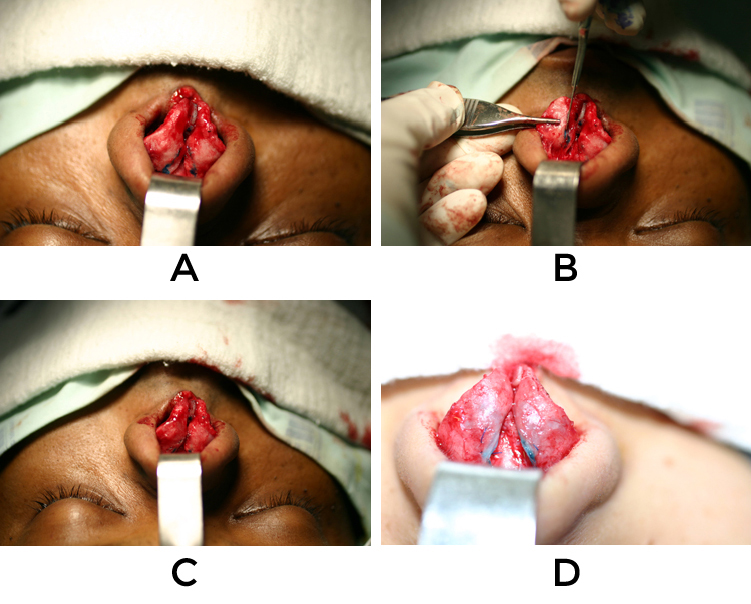
Columellar strut: The columellar strut is used in the surgical cases where an open approach is used to give additional support to the pedestal. This will help avoid loss of tip projection. The strut should be carved from a straight piece of cartilage. The first grafting option is septal cartilage although conchal cartilage or rib cartilage can also be used. The graft is placed in a pocket dissected between the medial crura.
It is sutured in place with absorbable 5-0 sutures taking care not to place these near the domes or high in the intermediate crural area in order to preserve the natural double break of the columella. The graft should sit a few millimeters above the nasal spine and should be cut slightly below the domes. Posteriorly the edge of the strut should not overlap the anterior portion of the caudal septum or the nasal spine because this will produce an uncomfortable clicking sensation at the base of the nose. The strut is designed to give additional support to the tripod and pedestal, helps maintain or increase tip projection and rotation, and corrects buckling or asymmetries that may be found in the medial crura. It also provides a stable base for the use of grafts in the nasal tip (Figure 6).
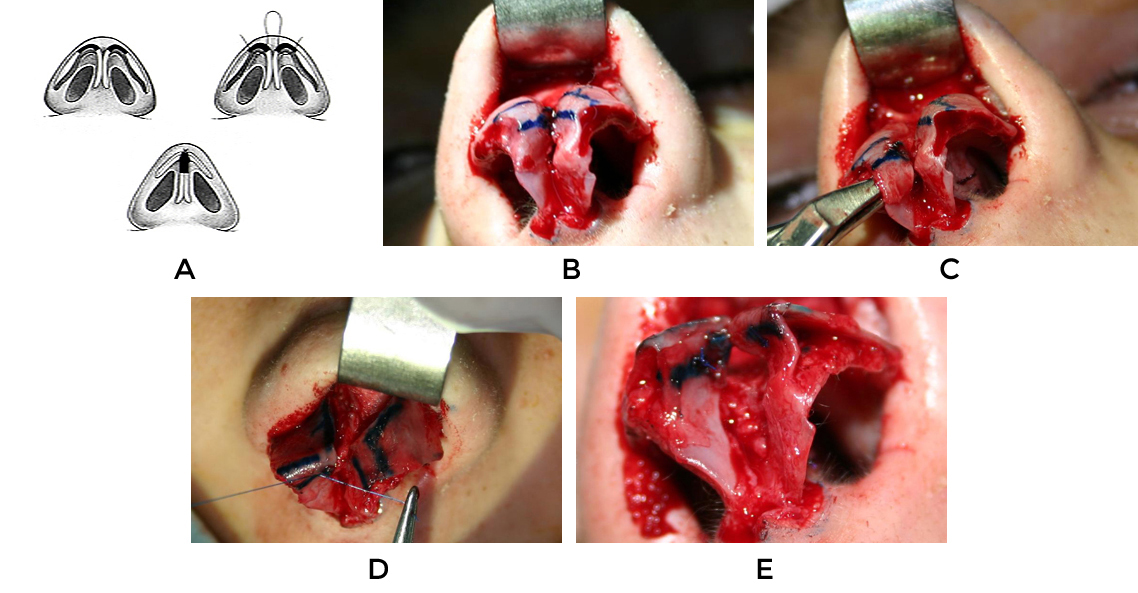
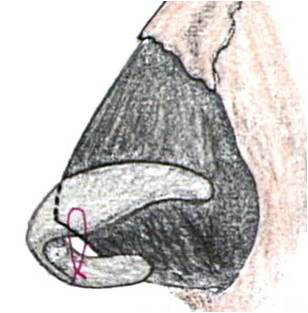
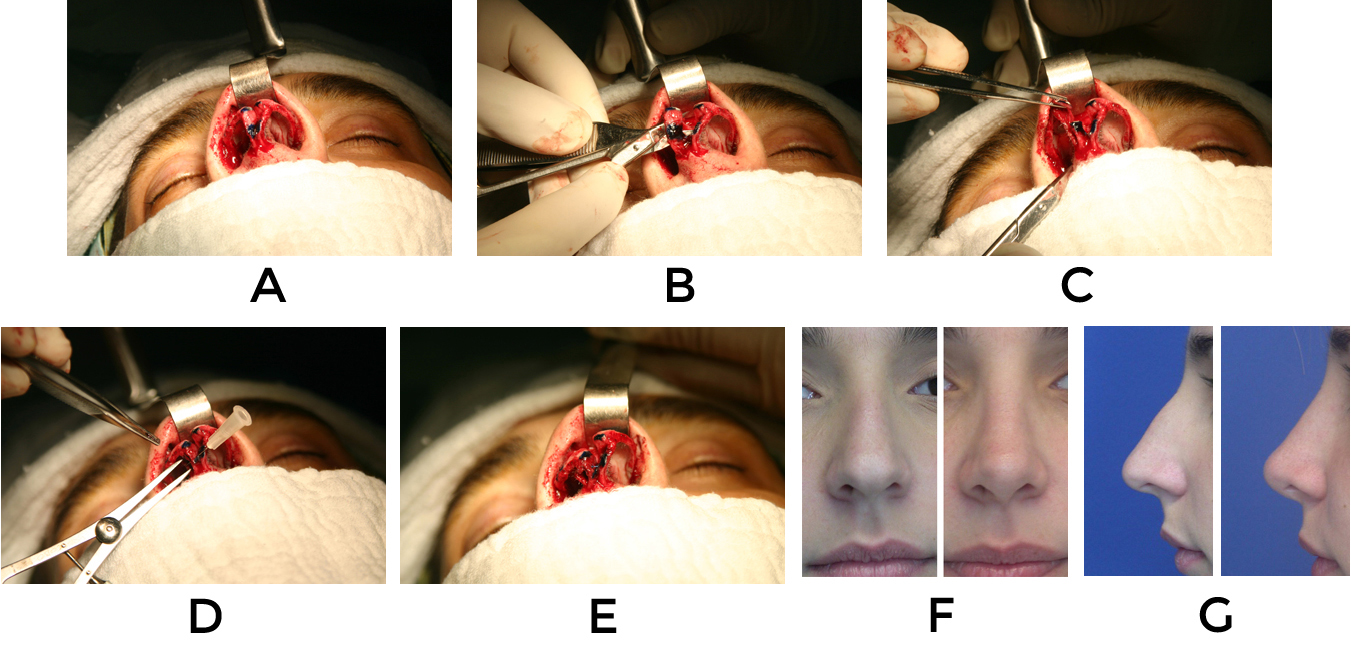
Caudal septal extension graft: Many times, the columellar strut will not give the necessary support the pedestal needs and will not correct big deformities in this area. The Caudal septal extension graft becomes very useful in these situations. The indications for its use are: patients with acute nasolabial angles, under projected tips, caudal septums that can be normal or short but with poor tip support or inadequate alar/collumelar relationships.18 The cartilage used in this type of graft should be relatively straight. The ideal material is septal cartilage, when this is not available, conchal cartilage can also be used although it is not as strong and the piece used should be straightened with sutures. The graft is placed overlapping for a few millimeters the caudal edge of the patient´s septum and sutured in place with 4-0 absorbable sutures. The graft must be fixed inferiorly at the level of the nasal spine and superiorly at the level of the anterior septal angle. If the piece of cartilage used reaches the region of the internal nasal valve, it should be thinned out so there won´t be a resulting nasal obstruction. Once the graft is fixed securely in place, the feet of the medial crura are sutured to the caudal edge of the graft. Where the feet are fixed will be defined by how much rotation and projection is needed. This position will define the final position of the nasal tip (figure 7).
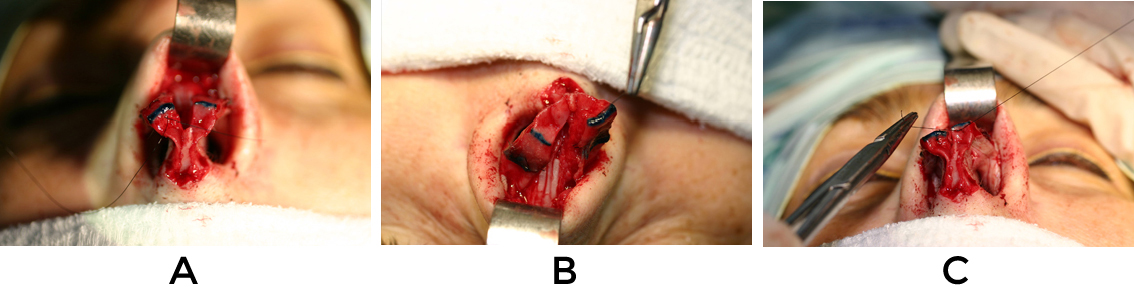
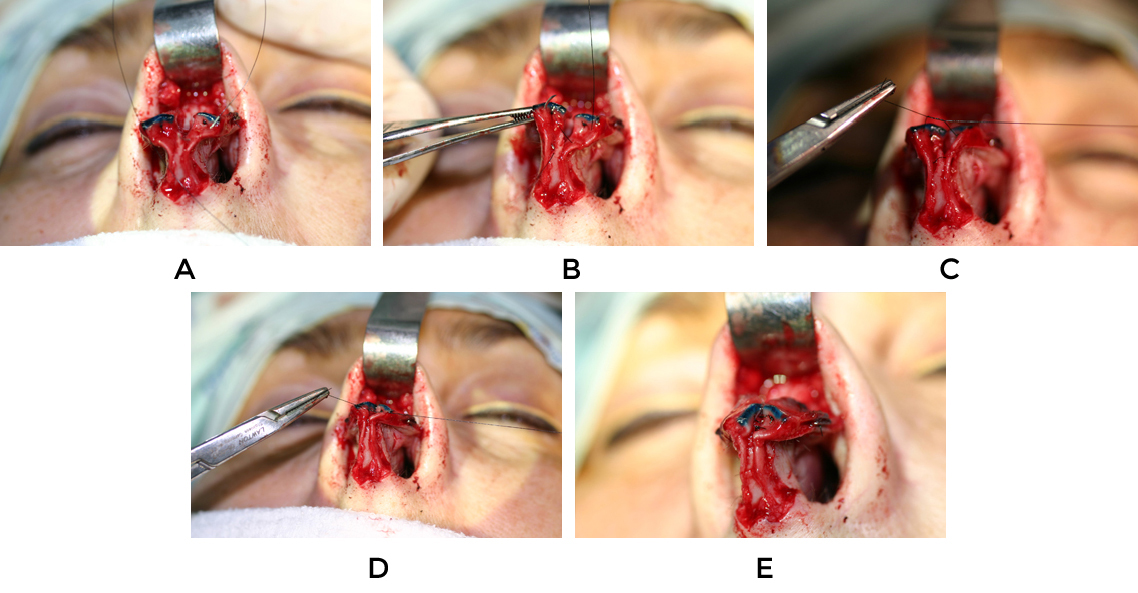
The shape of the caudal septal extension graft may vary. It usually has a rectangular shape, but in the patients where the nasolabial angle is very acute and rotation very poor, leaving the graft wider in the inferior portion will help push out this area and will help rotate the nasal tip superiorly (Figure 8, 9).
Gradual Approach to the Latino or Mestizo Nasal Tip
Once the nasal base has been strengthened and stabilized, the nasal tip can be approached. There are no standard procedures when working with mestizo noses. A gradual approach is used starting with conservative and predictable techniques leaving the more aggressive ones for prominent deformities. The tripod structure in Latino patients is more flimsy and unsupportive. Alar cartilages tend to be wide, with undefined domes, the feet of the medial crura are short, resulting in nasal tip lobules that are bulbous and lack projection and rotation.
The philosophy used in these patients is: minimal tissue resection, reinforcement of support structures of the nose, structural grafting, and use of sutures and grafts to help define and contour cartilaginous structures. As surgeons, we must be careful not to overuse grafts in these patients. We want nasal tips that look more defined without necessarily looking bigger. All sutures are performed with 5-0 non absorbable sutures being careful of burying knots so they will not extrude over time. 8
Problems encountered:
- Wide, flimsy alar cartilages
- Domes without definition
- Weak medial crura
- Rounded looking nostrils/ wide nasal base
Surgical techniques can be divided into intact strip procedures, incomplete strip procedures and use of grafts.
Intact Strip Procedures: These are procedures where the strip of alar cartilage is left intact and any changes performed are done with suturing techniques or with cephalic resection of the alar margin.
Cephalic resection of alar cartilages: In patients where alar cartilages are excessively wide in the vertical dimension (caudal to cephalic), a conservative cephalic trim leaving 9-10mm at the lateral crus and 5-7mm at the dome area can be performed. Resection should not be extended into the lateral portion of the lateral crus. This can result in supralar pinching or collapse of the lateral nasal wall that with time will tend to get worse. Cephaic trim is not performed routinely by the author. Tip bulbosity is usually dealt with suturing techniques to define the dome area and flatten any convexities that can be present in the cartilages.
Lateral crural turn-in-flap of cephalic portion of alar cartilage: In patients where the alar cartilages are very wide but additionally very flimsy and weak, instead of performing a cephalic resection of the alar cartilage, the portion that is going to be resected is folded under the cephalic edge and sutured in place. In this way the cephalic portion is strengthened and postsurgical pinching can be avoided (figure 10).
Suturing techniques: They are the first step in managing the bulbous undefined tip and are usually performed with 5-0 non-absorbable sutures. The big advantage of using suturing techniques is that if the result obtained is not satisfactory, things can be undone easily without major problems. Most suturing techniques are used to refine, project and rotate the nasal tip.
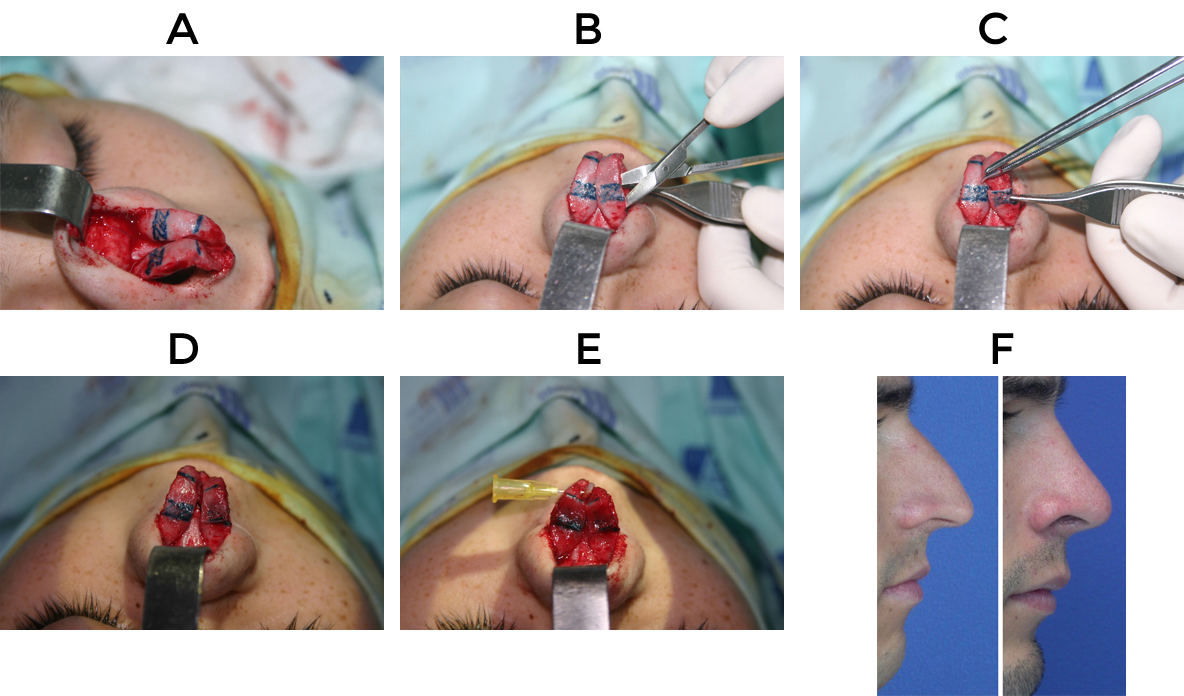
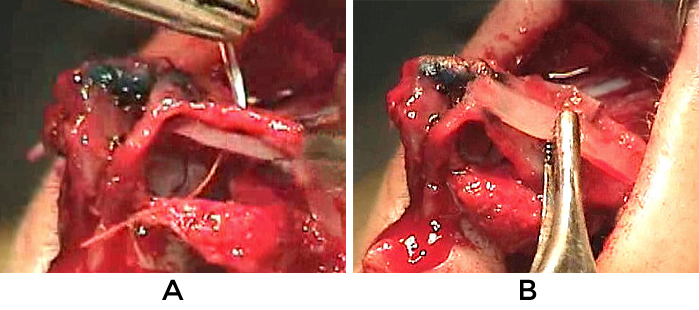
Lateral Crural Steal: This is one of the most useful techniques in mestizo noses because it increases rotation and projection without compromising support. The rotation is done by lateralizing the position of the domes by lengthening the medial crura. The vestibular skin of the alar cartilage is dissected from the undersurface of the dome area and the “new” dome is marked 3-5mm lateral to the existing dome depending on how much tip rotation is needed. This rotation is done by lenthening the medial crura at the expense of the lateral crura. Besides rotating and projecting the tip, this technique creates a more triangular base, and a tip with more definition (figure 11, 12)

Dome defining sutures: In the cases where the dome is in an adequate position but is not properly defined, mattress sutures are placed narrowing the domal angle. The suture must be tied trying to narrow the domal angle without pinching the domal area or producing buckling of the lateral crus of the alar cartilage. In the cases where the alar cartilage is very weak or a concavity forms after tying the sutures, the lateral portion of the cartilage can be straightened with a lateral crural strut graft (figure 13).
Intradomal Suture: This suture of 5-0 nonabsorbable material is performed to decrease the interdomal distance of the newly defined or existing domes narrowing a very wide nasal tip. Care must be taken not to suture the domes too close together as this can result in a “pinched” look or a unitip deformity. (figure 14)
Lateral Crural Spanning Suture: This is a mattress suture of 5-0 non absorbable material that is placed in the cephalic margin of the lateral crus of the alar cartilages and is tied in the midline. It helps improve and refine an extremely bulbous tip and helps correct an ala with marked hooding. It is important to try and avoid vertical tip malpositioning of the cartilages in an attempt to define and narrow the nasal tip (Figure 15).
The transdomal refinement suture: With this technique a 5-0 non absorbable mattress suture is passed through the existing domes and knotted in the midline. This suture changes the tip shape to a more triangular one (figure16). It is important not to tie the suture too tightly or to place the domes too close together. An adequate interdomal distance must be maintained to preserve the double light at the dome area.19
Septocolumellar suture: It is a loop suture that is introduced from a point low at the foot of the medial crura on one side, passed thru a point high in the caudal septum near the anterior septal angle, taken out at a point low at the foot of the medial crura of the contralateral side and then tied in the midline over the feet of the medial crura. This suture fixes the medial crura/columellar strut complex to the caudal septum and it helps preserve or slightly increase the rotation that has been achieved with other techniques. The nasal base must be stable and fixed in the midline so the whole complex will not be shifted to one side of the nose when the suture is tied in place (figure 17).
Division of alar cartilages: Long plunging tips with a very thick S-STE are not rare in latino or mestizo patients. These patients will have acute nasolabial angles with small and sometimes retrussive nasal spines accompanied by weak and short caudal nasal septums and long lateral and/or medial crura. In these patients a columellar strut combined with rotating techniques on the nasal tip will usually not be enough and the results won´t be long lasting because the pedestal will not have enough structural support. The surgical option that works well on these patients is the lateral crural overlay technique and the medial crural overlay. 20,21
Lateral Crural Overlay: Is very useful in long noses where the lateral crura is much longer than the medial crura. An incision on the alar cartilage is placed 10mm lateral to the dome. The segments are elevated and freed from the underlying mucosa and the medial segment is superimposed over the lateral segment several millimeters and sutured in placed with a 5-0 non absorbable suture. This technique shortens the length of the lateral crura, reinforces the lateral crus of the alar cartilage and rotates the tip upwards shortening the nose (figure 18).
Medial Crural Overlay: when the medial crura is overly long or very asymmetric a medial crural overlay is very useful. An incision is placed a few mm below the existing domes, and the fragments are superimposed and sutured in place with a 5-0 non absorbable suture. This creates counter-rotation of the nasal tip and lowers the height of the domes. In the cases where the overprojection is due to an overly long lateral and medial crura, an overlay technique in both areas of the alar cartilages will deproject the tip without changing the rotation (Figure 19).
Grafts: Grafts in the nasal tip can be grafts that give support and structure (structural grafts), they can be used to help define structures, or they can be used as camouflage . Mestizo or latino patients in general want noses that look smaller and have more definition. Additionally, these are noses that have poor osteocartilaginous support structures and a thick S-STE. It becomes very important to reinforce and build up structures to be able to create support and definition but without making them a lot bigger. Since the amount of cartilage available is limited, grafts should be chosen and used wisely. On the nasal tip, grafts should be placed carefully and when possible sutured in place to avoid post-surgical shifting.
Shield Graft: It is very useful in patients with thick skin that have bulbous, flimsy, undefined tips. Shield grafts can be shaped from septal, conchal or rib cartilage and should be carved according to patients needs. The graft is fixed in place to the caudal margins of the medial/intermediate crural strut complex with 6-0 non absorbable sutures. The leading edge of the graft should be positioned at the level of the existing domes or slightly above and covered with morcelized cartilage or perichondrium to prevent visibility of the leading edge of the graft over time. These grafts help improve definition and projection in the nasal tip. (figure 20)
Alar Strut Grafts: These are flat thin pieces of cartilage that are placed in the undersurface of the lateral crura. They will stiffen flimsy lateral crura, will help flatten the lateral crus when there is marked bulbosity or they can also correct any convexities created in the lateral crus when dome sutures are used. (figure 21)
Alar rim grafts: These grafts help correct alar contour irregularities, alar flare, and give the ala enough support to prevent collapse. They are thin, long pieces of cartilage that are placed in a non-anatomic position immediately above the alar rim. The graft should not extend all the way up to the soft triangle as this can create irregularities and asymmetries in this area.
When using the external approach, the graft is placed thru the marginal incision and its superior edge sutured in place with a 5 or 6-0 absorbable suture. The leading edge of the graft is crushed with a forceps or morcelized to prevent visibility over time. In Latino patients it is not unusual to find that there is a small convexity in the lateral crus of the alar cartilage after dome binding sutures have been performed. These grafts will help hide this irregularity and will give the nasal tip lobule a more symmetrical appearance. (figure 22)
Morcelized or Crushed Cartilage: Is cartilage used to hide and smooth out irregularities, fill in concavities and soften contours. Any cartilage can be used (septum, ear or rib) but septal cartilage is the ideal material for crushing. A cartilage/bone crusher is used trying to have as a result a piece of cartilage that is pliable, has the texture of a mat and will not break when manipulated. This cartilage is frequently placed over the supratip area to fill in any marked supratip breaks, over the alar cartilages covering the dome area, covering the leading edge of a shield graft or covering the nasal tip when tip suturing techniques have been used. Whenever possible it should be sutured in place with 6-0 sutures so it won´t shift over time. This type of graft is used frequently as a finishing touch in nasal tip surgery in latino patients even if they have a thick S-STE. This helps give a smooth round look to the nasal tip and helps hide any irregularities that could become noticeable over time (Figure 23). 8
Alar Base Reduction
Alar base reduction is not performed on a routine basis. If the nasal base is stabilized and the tip has increased its rotation and rotation, it is not infrequent to see that the orientation of the nostrils change acquiring a more normal and symmetric shape. This procedure is defined at the end of the procedure when all incisions have been closed. Incisions should be placed carefully to avoid unnecessary scarring. The medial incision usually is placed in the natural crease that is created between the nasal sill and ala. Laterally the incision should be kept within the alar facial groove if possible. Closure is performed using 5-0 or 6-0 non absorbable sutures taking care to evert edges. Sutures are removed after 8-10 days.
Skin Soft Tissue Envelope
Latino or mestizo patients tend to have a thicker S-STE . In spite of this, no defatting or thinning of the subcutaneous flap is performed. Cautery is used only when absolutely necessary as this can compromise the viability of the skin flap.
Postsurgical Follow-Up
Adequate follow-up on latino patients is a must. Columellar stitches and cast are removed after 1 week and nose is taped for an additional week. Excessive taping of the nose should be prevented as this will increase the inflammatory reaction on the skin.
Skin care is a priority in latino patients. Inflammation is more prominent and the skin covering the nasal dorsum and tip will be oilier and shinier several months after surgery. Sun exposure should be avoided for several months as this will increase edema. It is not uncommon to find dark circles under the eyes in mestizo patients. After surgery, these can become more prominent and it is imperative for patients to avoid sun exposure as this will definitely worsen pigmentation under the eyes. If the patient uses glasses or sunglasses, these should be avoided at least for 6 weeks after surgery. If glasses are needed, they should be taped on the forehead.
In the extreme cases where there is prominent acne that we know will worsen the postsurgical inflammation, it is important for them to follow a facial cleaning regime. In some cases these patients should be jointly treated with a dermatologist. When there is persistent edema in the tip or supratip region, this can be treated with 1-2mg injections of triamcinolone acetonide subdermically. Injections can be started as early as 2-3 weeks after surgery and can be repeated every 6 weeks, taping the tip area inmediatly after injection. Injections performed too frequently can result in permanent cutaneous atrophy, and it is important to reassure patients that inflammation will subside and skin will slowly regain its normal texture.
Rhinoplasty patients usually want to see immediate results in spite of the fact you have made them aware that real postsurgical results will not be completely appreciated until after 6 months to a year post op. It is important to have a good patient relationship established. This will help optimize final results and will definitely help during the initial postsurgical months.
Conclusions
Latino patients are one of the fastest growing ethnic group in United States today. Rhinoplasty is one of the cosmetic operations that is constantly asked for in this group of patients. Being able to establish a proper diagnosis and understand what our patients want is very important to be able to obtain consistent results. The most common problem found in these patients is a relatively weak structural bony and cartilaginous framework and a thick S-STE. These are noses that have problems with projection and rotation. Surgical techniques are focused on minimal tissue excision, strengthening of underlying support structures of nose and reorienting and increasing rotation and projection of the nose with sutures and grafts. The final result should be a nose that blends in with the patients face, does not change their ethnic features dramatically and can withstand the pass of time without resulting in important postsurgical deformities. The final goal of our surgery is to bring our patients closer to their aesthetic ideal but in a realistic fashion.
Bibliography
- The American Heritage Dictionary of the English Language, Fourth Edition Copyright © 2006 by Houghton Mifflin Company. Published by Houghton Mifflin Company.
- Ortiz Monasterio F, Olmedo A. Rhinoplasty on the mestizo nose. Clin Plast Surg 1977;4:89–102
- Ospina W. América Mestiza-El País del Futuro.Bogotá, Colombia: Villegas Editores; 2000. p.23–38.
- Milgrim L, Lawson W, Cohen AF. Anthropometric analysis of the female Latino nose. Arch Otolaryngol Head Neck Surg 1996;122:1079–86
- Cobo R. Mestizo rhinoplasty. Facial Plast Surg 2003;19(3):257–68
- Lawson, Hoefflin S. Ethnic Rhinoplasty. In: Hoefflin S. Ethnic Rhinoplasty. New York: Springer –Verlag; 1-15.
- Farkas L. Anthropometry of the Head and Face. 2nd ed.New York: Raven Press; 1994:286–301
- Cobo R. Hispanic/Mestizo Rhinoplasty. Facial Plast Surg Clin N Am 18 (2010) 173-188.
- Cobo R. Facial Aesthetic surgery with emphasis on rhinoplasty in the Hispanic patient. Curr Opin Otolaryngol Head Neck Surg 2008:16 (4):369-375
- Kim DW, Hwang HS. Traumatic rhinoplasty in the non-caucasian nose. Facial Plast Surg Clin N Am. 2010; 18: 141-151
- Toriumi D, Johnson C. Open rhinoplasty—featured technical points and long-term follow-up. Facial Plastic Surgery Clinics of North America 1993:(1)1–22)
- Becker D, Pastorek NJ. The Radix Graft in Cosmetic Rhinoplasty. Arch Facial Plast Surg 2001 3(2) 115-119
- Romo T. III, Abraham MT. The Ethnic Nose. Facial Plastic Surgery 2003: Vol 19, # 3: 269-277.
- Godin MS, Waldman SR, Johnson CM Nasal Augmentation using Gore-tex: a 10 year experience. Arch Facial Plast Surg 1999: 1(2) 118-21
- Toriumi D, Management of the Middle Nasal Vault in Rhinoplasty. 1995: Op Tech Plast Reconstr Surg. 2(1) 16-30
- Anderson JR: The dynamics of rhinoplasty. In Proceedings of the Ninth International Congress of Otolaryngology.Exerpta Medica International Congress Series, No. 206. Amsterdam, Exerpta Medica, 1969,pp 708–710.
- Johnson CM, To WC, The tripod-pedestal concept. In: A case approach to open structure rhinoplasty. 1rst Edition Philadelphia, Pennsylvania, Elsevier Saunders; 2005. P.9-20
- Toriumi DM. New concepts in nasal tip contouring. Arch Facial Plast Surg 2006: 8 (3)156–185
- Tardy ME, Cheng E. Transdomal suture refinement of the nasal tip. Facial Plast Surg 1987: (4) 317-326
- Konior RJ, Kridel R. Controlled nasal tip positioning via the open rhinoplasty approach. Facial Plastic Surg Clin of North America 1993: (1) 53-62
- Perkins S, Patel A. Endonasal Suture Techniques in Tip Rhinoplasty. Facial Plast Surg Clin N Am 17(2009) 41-54.