Introduction
Asia is a big continent, nose morphology changes from different regions. Often times when Asian rhinoplasty is the topic, it is the Eastern Asian nose that is talked about. East Asia is geographically divided into Far East Asia and South East Asia; and the South East Asian noses are one of the smallest noses in the world.1
Rhinoplastic surgery in small Asian noses requires improving the bulbous tip, elongating the dorsum, counter rotation and projection of the tip. To achieve this goal a strong support system of the dorsal and caudal strut should be achieved. The support grafts that works well are the extended spreader graft (ESG) and septal extension graft (SEG). Columellar strut graft when used alone will not give longevity of result because of weak lower cartilage coupled with the weight of the thicker fibrofatty skin. Improving the nasal morphology involves aggressive soft tissue contouring too by trimming the fibrofatty tissue. The ala is usually wide and hanging; this deformity has to be corrected as well. Therefore, in dealing with small Asian noses, 2 main surgical categories are considered: 1. Structural framework surgery e.g. support and contour grafts, and 2. Soft tissue contour surgery e.g. defatting the tip, alar lift and alarplasty.2
Structural framework surgery
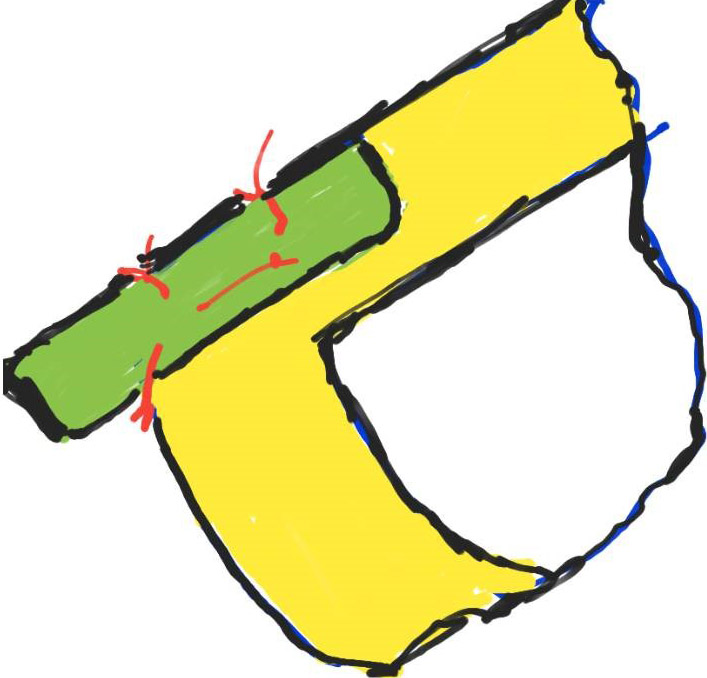
In the structural framework surgery, grafts are taken from septum. It is the SEG that is the strongest and has the longevity of tip support. There are many ways to design a SEG. Most commonly known are the “side to side” and “end to end”. See Figure 1 and 2.
The side to side SEG can be a full or partial overlap of the caudal strut depending on the strength of the caudal strut. If the caudal strut is weak, then a full side to side SEG is used to serve as a batten graft also. If the caudal strut is strong, then a smaller side to side SEG can be used. Extended spreader graft (ESG) is used when the dorsal strut is weak or deviated. See Figure 3.


Sometimes when the harvested septum is small, the ear cartilage is fashioned as extender of the support grafts.3,1 Occasionally the bony septum is used as support for weak SEG.4 See Figure 4, 5, 6,7




Synthetic material like polycaprolactone (PCL) can be used as support and template for cartilage growth whenever the septum is weak or small. See figure 8.
PCL mesh is a new absorbable synthetic material that has tissue regenerative property. PCL should be covered with cartilages in order to prevent extrusion or erosion to mucosa and to allow cartilage cells ingrowth.
The dorsal and tip grafts are fashioned after the framework structure is done. Synthetic dorsal implant is still the preferred choice because of volume and ease of shaping.

Soft tissue contour surgery
In the soft tissue contour surgery, attention is mainly at the fibrofatty skin of the tip, subtip and ala. The fibrofatty tissues at the supratip and alar crease are trimmed using sinus thru cut forceps at the end of the procedure. See figure 9.


If the subtip area is still big at the end of the surgery, an ellipse of skin in the subtip is excise, this maneuver somehow raised the nostril apex hence improving the nostril shape as well.5 See figure 10.


One aspect in soft tissue contour surgery is the Ala. The ala should be approached in 3 dimensions. Alarplasty addressed the 2 dimension of the alar flare and alar width. See figure 11.


The 3rd dimension is the alar rim which has to be raised since most Asian noses have hanging ala. The alar rim lift is done internally via sail excision.6,7 See figure 12.


This procedure involves removal of a triangular skin tissue with its subcutaneous fats and muscles then the alar rim skin is rolled in to close the defect. The fixed landmarks to follow are the vestibular groove and the inner margin of the alar rim. The alar rim lift via sail excision is done as initial step before rhinoplasty while the alar base and flare surgery is done as final step when rhinoplasty is done.
Conclusion
In conclusion, surgery of small Asian bulbous nose needs a strong structural framework and an aggressive soft tissue contouring surgery. See figure 13 and 14








References
- Yap, EC. Aesthetic Rhinoplasty for South East Asians, In: Jin HR. Aesthetic Plastic Surgery of the East Asian Face. 2016. 108-121
- Yap, E.C. Principles of Structural Rhinoplasty in South East Asian Noses. Philipp J Otolaryngol Head Neck Surg 2014; Jul-Dec 29(2): 41-44
- Pernia, N E, Galvez, JA, Victoria, FA. The Dimensions of the Nasal Septal Cartilage: A Preliminary Study in Adult Filipino Malay Cadavers. Phil Journal of ORL-HNS. Vol 26, No. 2, July-December 2011, 10-12
- Que-Ansorge, C., Yap, EC. The Use of Bony Septum as an Extended Spreader Graft in Primary and Secondary Rhinoplasty. Philipp J Otolaryngol Head and Neck Surgery 2019. Jan-Jun 34(1) 20-25
- Yap, EC, Rhinoplasty for South East Asian Nose. In: Jang, YJ. Rhinoplasty for the Asian Nose. Facial Plastic Surgery Clinics of North America. Aug 2018, 26(3) 389-402
- Baladiang DE, Olveda MV, Yap EC. The “sail” excision technique: a modified alar lift procedure for Southeast Asian noses. Philipp J Otolaryngol Head and Neck surgery 2010 Jan-Jun; 25(1): 31-37
- Yap, EC. Improving the hanging ala. Facial Plast Surg. 2012 Apr; 28(2): 213-217
Disclosure: There are no financial or other relationships, that might lead to a conflict of interest.