Abstract / Synopsis
Race and ethnicity have no scientific or anthropologic validity, yet nasal plastic surgeons continue to categorize patient demographic variables according to racial and ethnic lines. Ethnicity tends to include race but is also dependent on culture, language, religion, and nationality. Here we discuss the most common features of the Middle Eastern nose (MEN). There is great variety in anatomical characteristics and require careful surgical planning. A variety of noses are examined and critical steps are discussed.
Introduction
Rhinoplasty remains one of the most challenging operations, as exemplified in the Middle Eastern patient. Middle Eastern rhinoplasty (MER) is becoming more frequent, not only in the west in general and in the United States in particular but also in the region as more people break the cultural barrier locally and get international; mostly western exposure. This has meant a huge number of patients spend a huge amount of time and money on cosmesis. This can be seen by the many number of beauty centers seen in every major city of the Middle East providing services ranging from holistic medicine to facial and body contouring procedures.
Mature patients often request a more refined, feminine nose, whereas younger patients (aged 15 to 25 years) want a smaller, cuter nose. When patients consider cosmetic facial surgery, a multitude of factors surround their decisions, ideas of beauty change depending upon the social and cultural zeitgeist. The concept of beauty is and always will be subjective. In the past, tandardized mathematical proportions have been used, such as “phi mask” of Marquardt.
This mask is a model based on the golden, or “phi,” ratio found in beautiful things in nature and validated by a large database of attractive faces. Modifications were made to include not only a Caucasians versions but also African and Asian versions, these models are incapable of including the full range of ethnicities that often present to the facial plastic surgeon. Nevertheless, there are some characteristics of beauty that are agreed upon across race and gender.
These features include symmetry and a composite of average facial features.
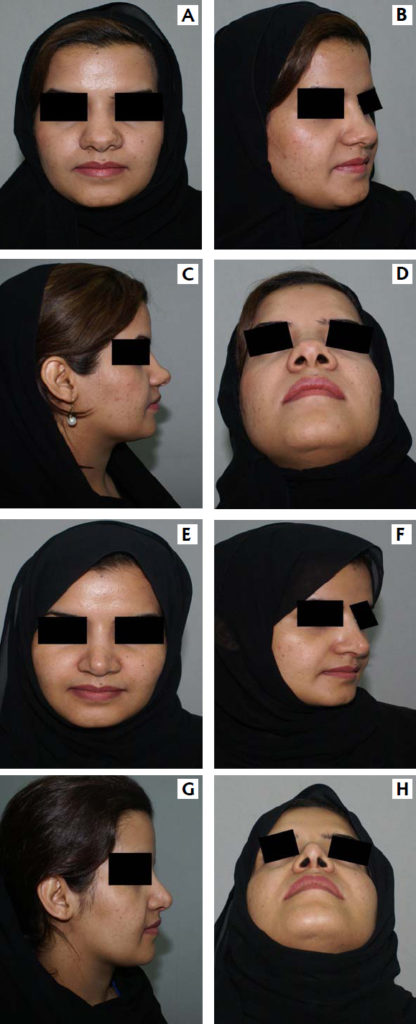
This patient has a typical middle eastern nose with boxy tip, wide alae, wide dorsum and deviated profile. A,B,C,D are pre-operative and E,F,G,H are three months post-operative results. This patient underwent open procedure with dorsal correction, tip work, bilateral spreader graft, columellar support and bilateral osteatomies.
Operative Techniques
The fundamental concept is to set the ideal profile line first and then create the desired tip. The procedure usually consists of the following sequence:
1) open approach with optional skin de-fatting, 2) tip analysis, 3) dorsal reduction and modification of caudal septum anterior nasal septum (ANS) as indicated, 4) septal surgery including septal cartilage harvest, 5) osteotomies, 6) insertion of spreader grafts, 7) columellar strut and tip sutures, 8) tip and radix grafts as needed, 9) closure with alar base modification as indicated, and 10) alar rim grafts as necessary.
Obviously, only those steps are done that are indicated, and other steps are added if necessary. Procedure becomes a “functional reduction” rhinoplasty as most MEN are bigger than the ideal.
Skin Envelope
Quite surprisingly, the majority if the Middle Eastern patients have normal to slightly thick than normal skin thickness, which requires no direct modification of the skin envelope. About one third of patients have thick, heavy, sebaceous skin, in which case lobular skin envelope de-fattening by dissecting in the subdermal plane would be necessary. Care as always needs to be taken to avoid being close to the dermis.
The Dorsum
Surgical planning for the dorsum involves the radix relationship and intrinsically height and base width of the osseocartilaginous vault. Dorsal reduction Is done in an incremental fashion using rasps for the bony vault and scissors for the cartilaginous vault.
The dorsal hump in Middle Eastern patients vary widely, the greatest reductions are done in the cartilaginous hump, which makes spreader grafts essential to avoid an inverted-V deformity.
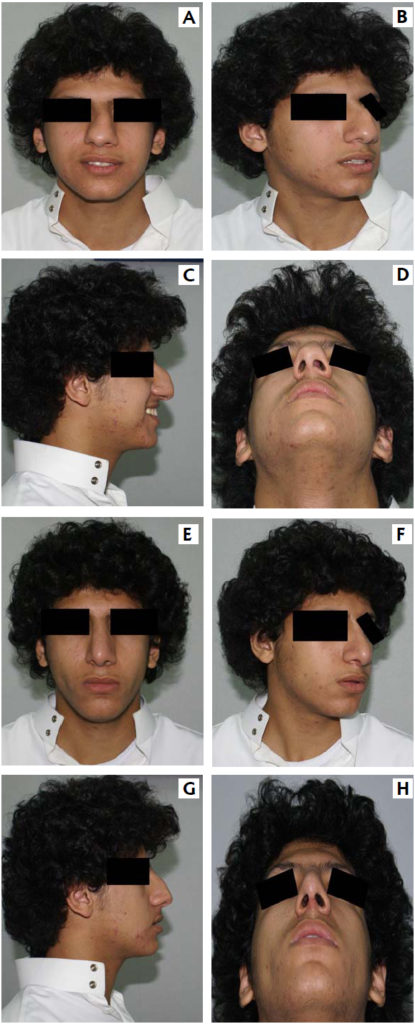
The usual appearance of Middle Eastern nose following nasal trauma during childhood. Pre-operative A,B,C,D as compared to one month postoperative
E,F,G,H.
Upper Lateral Cartilaginous
One unique anatomic finding is the extreme width of the upper lateral cartilages. Surgically, it is necessary to disrupt the lateral junction between the upper lateral cartilage and the lateral crura either by resection of excess cephalic lateral crura or by a sharp direct division with cartilage preservation.
Alar cartilages
Generally mid east alae are larger in comparison to the Caucasian ones. Hence the wide and heavy tip. Almost all cases require columellar struts to prevent the tip from drooping particularly while smiling and for support.
Alar Base
Most of the MEN’s have a wide and big alar base which would require alar basal resection, but not as much as those required by the black, asian or Hispanic group.
Septal Deviation and Asymmetry
Significant caudal septal deviation as well as bony-cartilagenous vault is almost always present. Asymmetry of the face in general is also very common.
Rarely do we come across cases where surgery can be done without osteotomies, which in many cases need to be asymmetrical.
Asthetics
Functional preservation may be the priority for us surgeons during surgery but most of the MER patients have strong opinions about their aesthetic goals and outcomes. While the older patients tend to feel their noses to be large with boxy, droopy tip and a deviated profile, the younger want good tip projection and rotation with a slightly curved bridge.
Most of the younger patients have a particular nose in mind before the come to the surgeon.
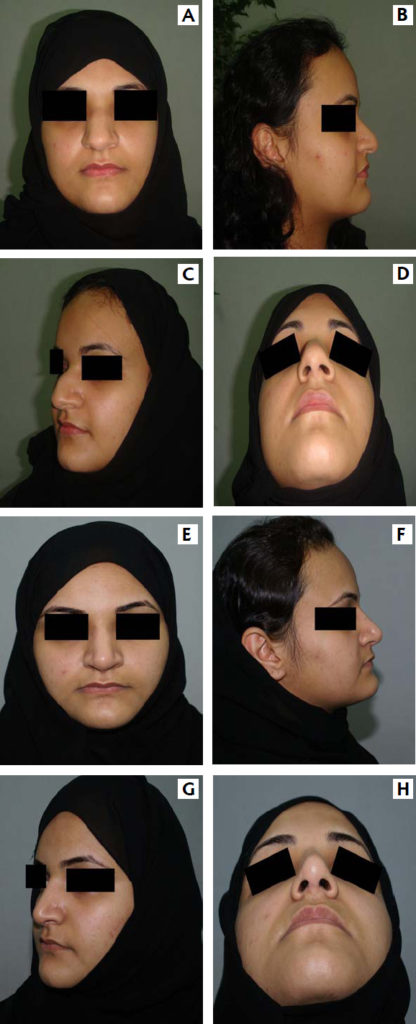
Patient with the most common nasal findings in the Middle East, particularly the arab world. Big nose, wide dorsum, bony-cartilagenous hump, bulbus tip with wide and asymmetric alae. She underwent open septorhinoplast. A,B,C,D – preoperative & E,F,G,H, – one month post operative.
Findings
Unfortunately, many of the cases here have been to the plastic surgeon for primary assessment or their first surgery. Many of our revision cases tend to be referred to us for functional correction and with persistent deformity after having had primary surgery by the plastic surgeon.
Principles
There are a few principles that need to be discussed for surgeons who rarely operate on MEN.
Since the Middle East is at the crossroads of the world, the people here are a mix from around the world and hence vary widely, unlike the Caucasians.
Hence they are not a homogenous subset of rhinoplasty and hence require through pre-operative analysis and great surgical planning. The patient expectation is usually very high with very specific needs, hence surgeon needs to spend time with the patient and discuss all steps and procedures and expected outcomes, if necessary with imaging programs to agree upon the final outcome.
- Expected findings and the actual anatomic findings usually are very different with significant variation.
- Usually the skin is thick and hence grafts are required as well as basal alar resection may be required in most cases.
- Destructive tip work techniques like alar resection etc look good immediately preoperatively but have poor long term results.
- Aggressive de-fattening is not warranted most of the times. Care needs to be taken not to go close to the dermis.
- Nasal shortening is essential, either by the ‘tongue in groove’ technique or direct resection of the caudal end or anterior septal angle.
- Dorsal hump is almost always present, both cartilaginous as well as bony which need to be removed appropriately, but as always, conservatively.

Pre-operative findings in A,B,C,D, & one month postoperative outcome in E,F,G,H.
Conclusion
In conclusion, the Middle Eastern nose is probably one of the most challenging types for rhinoplasty. Careful assessment and discussion preoperatively with the patient about outcome and limitations of surgery usually has a very satisfactory and favorable outcome postoperatively. The patient here have great interest in the procedure and they are a delight to work with once you see beyond the cultural inclination to bargaining and great obsession to detail.
References
Leong S. C, Eccles Ronald, Race & Ethnicity in Nasal Plastic Surgery: A Need for Science Facial Plast Surg 2010; 26:63-68
Rolling K. Daniel, Middle Eastern Rhinoplasty: Anatomy, Aesthetics, and Sur gical Planning. Facial Plast Surg 2010;26:110-118.
Hans Behrbohm, M. Eugene Tardy,Jr., Essentials of Septorhinoplasty, Phi losophy-Approaches-Techniques.
Angela K. Sturm-O’ Brian, Annette E. A. Brisstt, Anthony E. Brissett, Ethnic Trends in Facial Plastic Surgery. Facial Plast Surg 2010; 26:69-74.
Armando Brocciesi, The Surgical Approach to the Mediterranean Nose. Fa cial Plasty Surg 2010:26:119-130.