1. Anatomical characteristics
As a result of the diverse ethnicities in Asian populations, the anatomic characteristics of Asians vary greatly. Although there are substantial variations, in the typical Asian nose, the nasal skin tends to be thicker than Caucasian noses, with abundant subcutaneous soft tissue. The tip of the nose is usually low and the lower lateral cartilages are small and weak. The nasal bones are poorly developed and thick, thus having low radix. The septal cartilage is thin and small. The amount of harvestable septal cartilage is usually insufficient for simultaneous use for multiple grafts.1 Altogether, when compared with Caucasian noses, the typical Asian nose appears to be relatively small and flat, and has poor tip definition. In aesthetic analysis of nasal profile, the nasolabial angles of the Asians are typically more acute than those of Caucasians, but the nasofrontal angles did not differ greatly.2
2. Dorsal augmentation
General consideration
Dorsal augmentation is the most commonly addressed issue in Asian rhinoplasty and also the most common reason for revision surgery. When performing augmentation rhinoplasty on Asians, it is preferable or mandatory to first perform tip surgery using autologous cartilage, followed by dorsal augmentation using available implant material. The thickness of the patient’s skin must be taken into consideration. If excessive dorsal augmentation is performed on a patient whose skin is too thin, there is a risk of implant visibility through the skin or an extrusion of the implant. Conversely, too thick skin can decrease the effect of nasal augmentation. Therefore, in patients with thin skin, it is preferable to use soft implants such as Gore-Tex or autologous tissues such as morselized cartilage or fascia rather than silicone. In patients with thick skin, a relatively solid material such as silicone, reinforced Gore-Tex, or costal cartilage can be used without significant problems. In particular, when using implants with a certain level of hardness, such as silicone or costal cartilage, the base of the implant should be trimmed well so that it conforms to the contour of the nasal dorsum. Otherwise, an up and down motion by palpation or deviation of the implant can occur, leading to implant visibility through the skin.
Selection of implant material
1) Autologous Tissue
The advantage of autologous material for the dorsal augmentation of the nose cannot be questioned as these implants are well tolerated and carry the least risk of infection. However, if any autologous tissue other than septal cartilage is selected, the additional operative time required to harvest the graft and donor site morbidity become limiting factors. Common autologous tissues used for dorsal augmentation include septal cartilage, conchal cartilage, costal cartilage, fascia, and dermofat. As it is easy to harvest and shape the septal cartilage, it can be used to moderately elevate the nasal dorsum, to camouflage a partial concavity on the dorsum, and for nasal tip surgery. Since Asian patients have relatively small septal cartilage, it is practically difficult to harvest enough amount of septal cartilage, leaving at least 1cm width of the L-strut, suitable for a full length dorsal graft. In author’s study, dorsal onlay grafts with a width of 8 mm and preferred length of 30 mm could only be harvestable only in 9.1% of patients.1 To reduce the visibility and migration of the septal cartilages, and to overcome the limitation in the size, the author prefers to place the septal cartilage onto the nasal dorsum after gentle crushing using a cartilage crusher. Unlike septal cartilage, conchal cartilage has an intrinsic curvature that hampers its routine use as a dorsal augmentation in its original shape. In addition, the conchal cartilage is frequently too small to yield a cartilage piece suitable for one piece dorsal augmentation. When using conchal cartilage, it may be necessary to overlap pieces of cartilage in their opposite directions of curvature to neutralize their intrinsic curvature. Although costal cartilage is difficult to harvest and is associated with more serious donor site morbidity such as pneumothorax, as well as the problem of warping, it is the most useful autologous cartilage for substantial augmentation or in patients who have experienced complications with alloplastic implants.
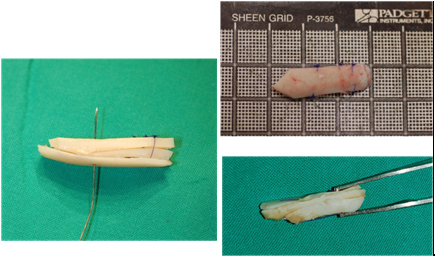
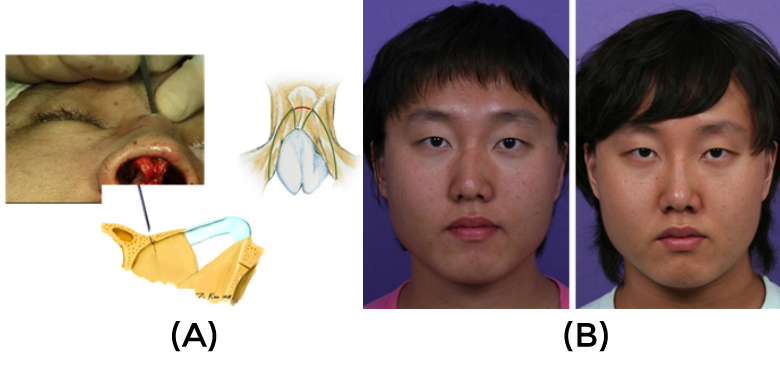
3 Although strongly advocated by some surgeons of its routine use for Asian rhinoplasty during the primary rhinoplasty, 4 however, it is very difficult to persuade Asian women to use costal cartilage because the harvesting procedure leaves scars on the chest. One other critically important limitation of autologous costal cartilage is that, except for only a few highly-experienced surgeons, most rhinoplasty surgeons have difficulty using these implants to create an aesthetically pleasing nose. Warping, graft visibility, and unnatural looking noses are common complications of augmentation using costal cartilage. (Fig.1)

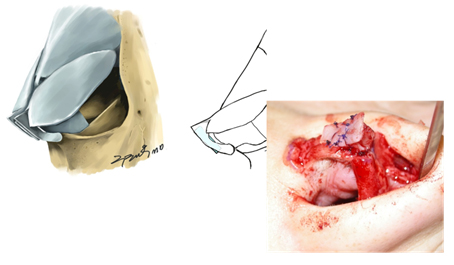
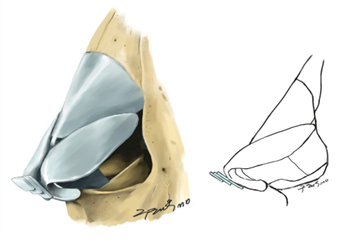
To avoid warping, it is best to soak the cartilage in saline solution to let the maximal warping occur, and perform careful carving after a certain time elapsed. To reduce the risk of warping, the author prefers to use costal cartilage in a laminated form. (Fig.2,3)

Although autologous cartilage has the lowest risk of infection among graft materials, autologous cartilage including costal cartilage is associated with a significant risk of revision surgery, with rates as high as 15.5 %.5 The primary reasons for this high revision rate is that autologous tissue is usually used to treat more difficult cases and use of these implants is associated with unpredictable scarring, warping, and at times visible graft contours. Although, harvesting autologous fascia requires an additional incision and hence is associated with additional morbidity, autologous fascia, including temporalis fascia and fascia lata, can be used in rhinoplasty as radix graft or dorsal onlay grafts. Fascia can be used alone or can be used as a form of fascia wrapped diced cartilage, which can maximize the full use of the small pieces of autologlous tissues remained after other procedures, can nicely camouflage dorsal irregularity or, could serve as an alternative method of dorsal augmentation.6 Studies have shown that diced cartilage-fascia wrapped grafts survived and demonstrated normal cartilage survival.7 Dermofat, harvested from various locations, can also be used in dorsal augmentation. Although dermofat can be harvested in great quantities, its absorption is difficult to predict, making it unsuitable for substantial dorsal augmentation. However, dermofat can be useful for patients with thin skin or contracture of the nose due to complicated primary rhinoplasty.8
2) Homologous tissue or tissue allograft
Homologous costal cartilage, which is not associated with harvesting morbidity or additional operation time, could serve as an alternative graft material. For example, homologous costal cartilage harvested from cadaveric donors and processed in various ways has been shown to be useful in rhinoplasty.9-11 Homologous costal cartilage can be used in revision rhinoplasties requiring structural reconstruction of the nasal framework, but in which patients resist harvesting their own costal cartilage. The use of homologous costal cartilage in rhinoplasty has shown conflicting results regarding the degree of resorption and warping. 9-11 In the author’s own experience, a significant numbers of patients had unpredictable complications such as resorption, warping, and graft visibility when this cartilage was used as full-length dorsal graft. The high complication rate associated with homologous cartilage may limit its utility for dorsal augmentation.
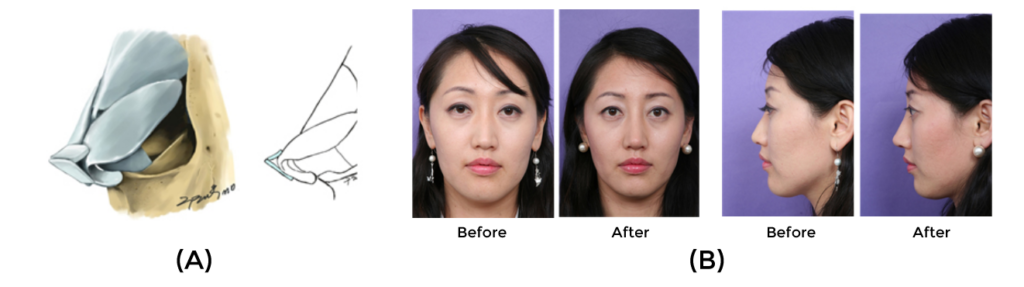
Tutoplast processed fascia lata (TPFL) is commercially available homograft fascia that has been successfully used as human tissue grafts in various purpose. 12,13 The author has used TPFL in rhinoplasty for dorsal and radix onlay grafts. TPFL can be used for smoothening grafts for dorsal irregularity following correction of a deviated nose, as additional graft material when an inadequate amount of septal or conchal cartilage is available for dorsal augmentation, in patients who dislike using of alloplastic material for dorsal augmentation, for complicated revision surgery in which silicone has been used on the dorsum. (Fig 4,5)
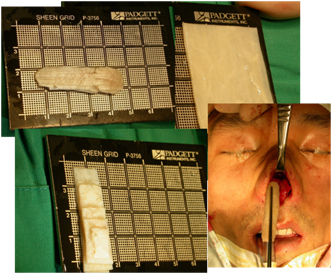

Combined use of crushed cartilage and TPFL is also an effective technique for dorsal augmentation that can achieve a significant degree of dorsal augmentation. This technique provides surgeons and patients who prefer autologous cartilages with favorable and predictable outcomes in rhinoplasty.14 ( Fig.6,7)


The soft contour of TPFL means that it can be nicely blended with the overlying skin soft tissue envelope. Although TPFL has very low risks of infection, displacement and extrusion, but an unpredictable degree of resorption could be a problem.13
3) Silicone
Nasal dorsal augmentation with silicone rubber is the most popular rhinoplasty procedure in Eastern Asia. Due to its stable chemical structure, silicone has several advantages including its lack of tissue reaction and ease of handling. Moreover, the availability of ready-made products makes application convenient and the relative hardness of silicone makes it suitable for fashioning the desired nasal shape for Asians with a thick skin.15,16 The skin of Asians is thicker than that of Caucasians, so there is a lower risk of an implant extrusion after surgery. The prefabricated products can be divided largely into L and I shaped implants. Some surgeons favor an L-shaped or a variation of I-shaped silicone (covering the nasal tip) capable of covering from the radix all the way down to the nasal tip.

However, because the nasal tip area is an area that is always exposed to exterior stimulation, the use of L-shaped silicone carries a higher risk of extrusion, regardless of the thickness of nasal subcutaneous tissue in Asians, Thus, a placement of I-shaped implant at the nasal dorsum area and tip plasty using an autologous material (septal cartilage, conchal cartilage) at the nasal tip area is preferable surgical method. In addition to using prefabricated silicone implants, the author has used silicone sheeting for nasal dorsal augmentation, which is more versatile but without an increased risk of complications.17(Fig.8)
In trimming the silicone, it should preferably be about 3.5~4.0cm long and about 8mm wide and the edge should be as thin as possible. To insert the silicone, the size of the pocket should be made slightly larger than the implant, with just enough space for insertion of the implant and a surgical tool holding the implant at the same time. Revision rhinoplasty after silicone implants may be needed for implant deviation, floating, displacement, extrusion, impending extrusion, and infection.16 (Fig 9) Although infection is one of the most dreadful
Figure 9. Patients’ photograph showing complication of rhinoplasty using silicone. Alar retraction with implant extrusion was corrected with autologous cartilage grafting
complications of silicone implants, early infections can be prevented by the use of aseptic techniques and prophylactic antibiotics. Infection can also be treated by implant removal, antibiotic administration, and delayed reinsertion. Extrusion of the implant can occur through the nasal skin or mucosa, with tension over the implant being the most common cause of extrusion.
4) Gore-Tex
Gore-Tex (expanded polytetrafluoroethylene:ePTFE), next to silicone, is the most widely used alloplastic implant in Asian noses, and currently it’s use is on the increase. Gore-Tex implants are porous inducing the surrounding tissue to grow inward through the pore, and have the advantages of increased stability and lower incidence of capsule formation. In addition, the risk of extrusion is lower with Gore-Tex than with silicone. The soft texture of Gore-Tex reduces patient discomfort and the occurrence of unnatural visible implant contours through the skin.(Fig 10) One important disadvantage of Gore-Tex is that it decreases in volume after insertion. In addition, it is more difficult to remove a Gore-Tex implant than a silicone implant.
Reports of a delayed inflammation (Fig. 11) are increasing and outcome data are not adequately accumulated to date. One must be cautious when using Gore-Tex in the
presence of inflammation within the nasal cavity (sinusitis, vestibulitis, and active acne). Moreover, when performing operations that may create micro-communication with the nasal cavity (e.g.osteotomy or septal reconstruction), there is an increased risk of infection. It has been recommended that patients be treated with antibiotics prior to inserting the Gore-Tex as well as after surgery, and it is essential to soak the Gore-Tex in saline solution containing Betadine or antibiotics before use. Also, before handling the Gore-Tex, surgical personnel should wash their gloves to remove powder or other foreign substances. It has been reported that infection rate in primary surgery is 1.2%, while infection rate in secondary surgery is 5.4%.18
3. Osteotomy
Osteotomy is an important technique for correction of a deviated nose, hump reduction, and modification of brow-tip aesthetic line. Although osteotomy can be used as frequently for rhinoplasty in Asians as in Caucasians, osteotomy for Asian noses carries a special challenge, due to the size and thickness of the bone. In Asians, the nasal bones are generally small and thick, thus increasing the risk of shattering the bone and fracturing it into small pieces. In these patients, alternative procedures, such as onlay grafts, are recommended in place of an osteotomy. In addition, percutaneous lateral osteotomy, which is widely performed during rhinoplasty in Caucasians,19 is not suitable for patients with thick and small nasal bones. It is difficult to make several holes in thick nasal bone, and to connect the holes using digital pressure. Thus the author recommends that medial and lateral osteotomy be formed using the internal continuous method, not the percutaneous route.
Also, among patients with excessively thick skin, a common trait in Asian populations, the changes induced by an osteotomy frequently do not appear externally, making the effect of osteotomy less prominent. Correction of a deviated nose is not possible if the direction of the midline bony septum left over from medial and lateral osteotomy is not straight. The midline bony septum should therefore be fractured to completely mobilize the midline structure. However, when the central bony structure is so thick as to resist fracturing by digital compression, a percutaneous root osteotomy can be performed to fracture the bony septum and relocate it in the desired direction.20 Percutaneous root osteotomy is performed at the eyebrow level using a 2 mm osteotome. (Fig 12)
As a prerequisite, the dorsal part of the cartilaginous septum must be separated from the upper lateral cartilages. At times, however, the severed bony segment can collapse towards the nasal cavity following a root osteotomy. In such cases, it is recommended that an onlay graft be performed using a bony fragment or cartilage.
4. Management of convex nasal dorsum
In contrast to the well developed and prominent noses of Caucasians, noses of Asians are generally small and less prominent. Accordingly, the prevalence of a hump nose among Asians is relatively low. Rhinoplasties for Asian noses had traditionally been over-simplified and over-represented as augmentation rhinoplasty using alloplastic material such as prefabricated silicone. However, this simple approach can not be a universal remedy for the various different aesthetic features presenting in Asian nose, particularly for the correction of dorsal hump. Humpectomy followed by osteotomy and tip surgeries are typically required for dorsal hump reduction for Caucasian noses. However, in the treatment of dorsal hump in the under-developed and under projected Asian noses, a rather different treatment strategy such as reduction in combination with dorsal augmentation may be required. When examining patients’ nose, I could easily find that there are typical hump as well as hump like deformity. Thus the author would collectively call the hump noses and hump variant noses into a convex nasal deformity.21 They require customized therapeutic plans for better management, and surgeon must well aware that the strategies for treating these patients, therefore, must vary accordingly. Generalized hump represents a typical hump seen in Caucasian population, in which the curvature of the hump begins from the bony vault and goes all the way down to the cartilaginous dorsum in a form of a gentle curve (Fig.13).
Isolated hump represents instances of abrupt protrusion of a small hump in a triangular or round shape at the dorsal line (Fig.14).
The total length of the hump is short and, when they are exposed to surgery; most of the hump can be found located around the rhinion. Relative hump with low tip (Fig.15)



represents the cases where the height of nasal dorsum is not so prominent, but instead, the nasal tip is underdeveloped, giving a false impression of nasal dorsal hump. In most cases of convex nasal dorsum, proper tip augmentation using suitable tip surgery techniques are of utmost importance for ultimate aesthetic success. When the patient presents low radix, augmentation of radix using crushed cartilage, resected hump, or fascia should be performed. Even in case of generalized hump, some patients want dorsal augmentation. In this case, augmentation of the cartilaginous dorsum, the level of which adjusted by newly created tip height was conducted to make an ideal dorsal profile line. Hump reduction can be performed either via open and closed approach. The author’s preferred technique is open rhinoplasty approach, which was particularly more useful in case of generalized hump, where several surgical maneuvers other than simple hump reduction were required.
The rationales for dorsal augmentation in hump management are: first, there are a number of patients requiring the correction of minor contour irregularity, thus requiring smoothening graft. Secondly, many Asian patients want augmentation together with reduction because they have relatively small, flat, and under-projected nose. In addition, most patients with convex nasal deformity need their tip elevated first, and then the dorsum should be elevated correspondingly in order to have a harmonious dorsal line. This is particularly true for the patients with low tip. Therefore, the author would suggest that the corrective operation of convex nose deformity for Asian is rather close to redistribution surgery rather than a simple reduction. Usually, the success rate of hump reduction is significantly higher in isolated hump group than in the generalized hump group and relative hump due to low tip. The authors has relatively high incidence of under correction, which might be due to conservatism in treatment.
5. Correction of deviated nose
The surgical principles applicable to the management of the bony vault, middle vault, and lower third of the Caucasian nose are also applicable to the correction of deviated noses in Asians.22 But, the problem in the management of this problem is that many patients lack sufficient amount of septal cartilage for simultaneous usage in reconstructing septal framework, tip surgery, and dorsal augmentation. Thus the surgeon frequently must harvest conchal or costal cartilage for complete correction of the deviated nose. In addition, many patients undergoing correction of a deviated nose also want dorsal augmentation as a result of surgery. Thus dorsal augmentation may be regarded as an important part in the correction of deviated Asian noses. Dorsal augmentation is performed during the last stage in the correction of a deviated nose. Through this procedure, the surgeon re-establishes the harmony between the bone and the skin soft tissue envelope as well as the balance between the function and the aesthetics of the nose. Some patients with deviated noses manifest contracture of the skin and soft-tissues in the severely deviated area. Proper dorsal augmentation can help overcome the deformity of the soft tissue that contributes to the formation of the deviation. In addition, dorsal augmentation itself helps the nose look longer and narrower. Surgical maneuver required for correction of deviated nose can create a micro-communication between the nasal cavity and the dorsum, increasing the risk of infection, when alloplastic implants such as Gore-Tex or silicone are used as dorsal implant. Thus choosing the ideal implant material becomes difficult. During the correction of a deviated nose, the author prefers to use material such as crushed cartilage or fascia because of its relative softness and its easy blending with the skin.
6. Surgery of the nasal tip
A careful observation of the nose of Asian noses reveals a surprising diversity in the shape of the nasal tip. Thus, various tip surgery techniques once thought to be applicable only to Caucasians are also largely applicable to Asians. The typical endonasal approach for the tip involves cephalic resection through delivery or nondelivery approach, and placements of transdomal and interdomal sutures and columellar strut. This approach can also be used for the placement of shield or onlay graft. Cephalic resection using the nondelivery approach is impractical for Asian patients, because tip surgery requiring only a cephalic resection is very rare in Asian patients. Meanwhile, a certain level of tip projection and rotation can be achieved through the incision on the skin from the middle crus of the lower lateral cartilage to the vestibule side.23 Using this limited marginal incision and subsequent dissection of the caudal area of the lower lateral cartilage can enable a surgeon to place the onlay graft at the tip area. The external rhinoplasty approach is a versatile approach that enables the surgeon to precisely diagnose nasal tip deformity and to tailor treatment using various tip surgery techniques.24 The most common of these tip surgery techniques include columellar struts: shield, onlay, and septal extension grafts: and transdomal, interdomal, and septocolumellar sutures.25-28 Selection of the specific maneuver is dependent on the shape of the patient’s deformity, the availability of grafting material, and the surgeon’s preference. Among the multitude of tip surgery techniques, followings have important role and should be emphasized for the Asian tip.
1) Septal Extension Graft
Although the under-projection of the tip among Asians frequently results from an inadequately developed lower lateral cartilage, it may also be caused by poor caudal septal support. If an adequate quantity of septal cartilage can be obtained after preserving its L-strut, this cartilage can be used as a septal extension graft to elevate the anterior septal angle of the septal cartilage as well as to strengthen the support.
29,30 As a result, the tip support can be strengthened along with the creation of a significant projection. One of the advantages of this technique is that, besides the projection/rotation of the tip, it can be useful in correction of the short nose deformity, which can be commonly found in Asian population. In particular, in patients with a retracted columella, a caudal extension of the graft can be particularly effective in improving the columellar retraction, as well as correcting the caudal septal deflection. Septal extension grafts can be classified into three types, depending on the graft.27 (Fig 16)

In performing septal extension graft surgery, it is preferable to position the graft at both sides of the caudal septal cartilage due to the reduced risk of causing nostril asymmetry, as well as the stronger nature of the grafting. In reality, however, it is difficult to obtain sufficient cartilage to place the graft on both sides and hence the procedure is generally performed only on one side.
2) Modified vertical dome division technique’
Vertical dome division(VDD) is powerful and versatile techniques for refining nasal tip aesthetics. VDD can be used for various nasal deformities, including overprojection or underprojection, suboptimal rotation, disproportionate lobule rations, and broad or asymmetric tips. Asian nasal tip require more structures to project into the thicker skin to gain the desired refinement because Asians have thick skin in comparison with that of Caucasians. Therefore, it is difficult to gain the desired nasal tip refinement using VDD alone in Asians. So, I modified this technique, and the most significant features of my modification of VDD technique were the way of dividing the domal region and the routine use of a tip graft to effectively refine the nasal tip.31(Fig 17,18)

The incisions on the domes were designed to borrow a large amount of cartilage from the caudal margin, so that the lateral view of the medialized cartilage had a triangular projection shape in an antero-caudal direction. The technique makes it easier to place an additional tip graft such a shield or onlay graft. The triangular shape of the medial limbs may not only increase projection of the tip but also stabilize the shield graft because the borrowed domal cartilage plays a role as the blocking graft. This technique is particularly suitable for patients with thick skin with strong and well-developed lower-lateral cartilages.
3) Multilayer tip grafting technique
Cartilage grafting is recognized as the most effective procedure in Asian patients, especially in cases requiring major tip refinement. Current tip grafting procedures include shield grafting, onlay grafting, cap grafting, and lateral crural onlay grafting. Vertically oriented shield grafts, popularized by Sheen, are widely used particularly for Caucasian patients. The horizontally oriented onlay graft placed on the dome area, popularized by Peck, is another effective method of enhancing tip aesthetics. The effectiveness of both of those procedures relies on the shape and orientation of the underlying LLC. However, the LLC shape and orientation in Asian patients is often not ideal for those procedures. An under-projected tip often presents with a round tip contour, and a vertically oriented shield graft or onlay graft can actually worsen the nasal tip shape. Therefore, it is not always possible to use procedures effective in Caucasian patients in Asian patients. In this scenario, a multilayer tip graft technique can be a nice technical alternative that can bring about desirable tip aesthetics.32 This technique is usually preceded by caudal extension of the septum, columellar strut placement, modification of the LLC, dome-suturing, and/or trimming of skin-soft tissue envelope (SSTE). Following those procedures, the first cartilaginous shield graft layer is placed on the dome. Further shield graft layers are then placed on top of the first layer. The more caudal layer is placed so that its leading (superior) edge is always higher than the height of the existing dome and the layer(s) beneath it (Fig.19,20).

The numbers of graft layers applied depend on how much projection was required, and was determined intraoperatively. The shield graft horizontal width is adjusted according to tip skin thickness. For thin skin, the horizontal width is wider to provide better tip definition. For thick skin, a narrower width provided better results. For evaluation of the final tip shape, the SSTE is redraped with interim stitching of the columellar incision. When the SSTE was redraped, it would usually push the grafts backward and could distort the tip shape and orientation. The author use one of two methods to prevent this from occurring: 1. if strong conchal cartilage was used as grafting material; I utilize its inherent concavity by facing the concave side caudally (Fig 21).

This allowed the natural antero-caudal spring-like effect to resist cephalic bending due to redraping of the SSTE. 2. For grafts which did not possess intrinsic curvature, such as septal cartilage, placement of a backing graft is mandatory. (Fig 22)
The backing graft is designed to span the horizontal dimension of the domal area, not exceeding the width of the dome. The present multilayer cartilaginous tip grafting technique could maintain the advantages of shield-shaped tip grafts which help to improve nasal tip projection and definition, and overcome issues relating to thick skin, soft tissue and weak cartilaginous framework often encountered in Asian rhinoplasty patients.
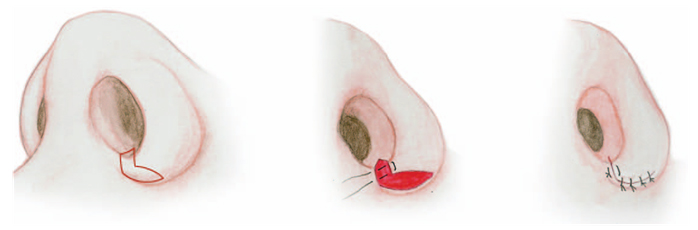
7. Alar base surgery
Since many Asian patients tend to have a broad alar base, alar base surgery is a very important supplementary surgical technique in Asian rhinoplasty that is used to construct a cosmetically balanced nasal base. Most alar base surgeries are performed to reduce the width of the nose and are known by an assortment of names, including as alar base reduction, alar base resection, and alar wedge resection.33 I prefer to perform alar modification usually by combined sill and alar excision technique. (Fig 23,24)

|
Player goes here
|
References
1.Kim JS, Khan NA, Song HM, Jang YJ. Intraoperative measurements of harvestable septal cartilage in rhinoplasty. Ann Plast Surg 2010;65:519-23.
2. Wang JH, Jang YJ, Park SK, Lee BJ. Measurement of aesthetic proportions in the profile view of Koreans. Ann Plast Surg 2009;62:109-113.
3. Guerrerosantos J. Nose and paranasal augmentation: autogenous fascia and cartilage. Clin Plast Surg 1991; 18: 65-86.
4.Toriumi DM, Swartout B. Asian rhinoplasty. Facial Plast Surg Clin 2007;15:293-307.
5. Bateman N, Jones NS. Retrospective review of augmentation rhinoplasties using autologous cartilage grafts. J Laryngol Otol 2000; 14:514-518.
6. Daniel RK. Diced cartilage grafts in rhinoplasty surgery: current techniques and applications. Plast Reconstr Surg. 2008 Dec;122:1883-1891.
7. Calvert JW, Brenner K, Dacosta-Iver M, et al. Histological analysis of human diced cartilage grafts. Plast Reconstr Surg2006;118:230-206.
8. Yang SJ, Kim BS, Kim JH. Secondary augmentation rhinoplasty with dermofat graft. J Korean Soc Plast Reconstr Surg1998;25:152-160.
9. Welling DB, Maves MD, Schuller DE, et al. Irradiated homologous cartilage grafts. Long-term results. Arch Otolaryngol Head Neck Surg 1988;114: 291-295.
10. Strauch B, Wallach SG. Reconstruction with irradiated homograft costal cartilage. Plast Reconstr Surg 2003;111: 2405-2009.
11. Lefkovits G. Nasal reconstruction with irradiated homograft costal cartilage. Plast Reconstr Surg 2004;113: 1291-1292.
12. Ghoniem GM. Allograft sling material: is it the state of the art? Int Urogynecol J Pelvic Floor Dysfunct 2000; 11: 69-70.
13.Jang YJ, Wang JH, Sinha V, et al. Tutoplast-processed fascia lata for dorsal augmentation in rhinoplasty. Otolaryngol Head Neck Surg 2007; 137:88-92.
14. Jang YJ, Song HM, Yoon YJ, Sykes JM. Combined use of crushed cartilage and processed fascia lata for dorsal augmentation in rhinoplasty for Asians. Laryngoscope 2009;119:1088-1092.
15.Tham C, Lai YL, Weng CJ, et al. Silicone augmentation rhinoplasty in an oriental population. Ann Plast Surg2005;54:1-5.
16. Erlich M, Parhiscar A. Nasal dorsal augmentation with silicone implants. Facial Plast Surg Clin 2003;19:325-330.
17. Wang JH, Lee BJ, Jang YJ. Use of silicone sheets for dorsal augmentation in rhinoplasty for Asian noses. Acta Otolaryngol 2007;127 Suppl 558;115-120.
18. Godin MS, Waldman SR, Johnson CM. Nasal augmentation using Gore-Tex: A 10-year experience. Arch Facial Plast Surg 1999;1:118-121.
19. Bull TR. Percutaneous Osteotomy in Rhinoplasty. Plast Reconstr Surg 2001; 107: 1624-1625.
20. Jang YJ, Wang JH, Sinha V,et al. Percutaneous root osteotomy for correction of the deviated nose. Am J Rhinol2007;21:515-519.
21. Jang YJ, Kim JH Classification of convex nasal dorsum deformities in Asian patients and treatment outcomes. J Plast Reconstr Aesthet Surg. 2010 Jun 28 in press
22. Gunter JP, Rohrich RJ. Management of the Deviated Nose: The Importance of Septal Reconstruction. Clin Plast Surg 1988; 15: 43-55.
23. Sheen JH. Tip Graft: A 20-year Retrospective. Plast Reconstr Surg 1993; 91: 48-63.
24. Adamson PA. Open Rhinoplasty. Otolaryngol Clin North Am 1987; 20: 837-52.
25.Behmand RA, Ghavami A, Guyuron B. Nasal Tip Sutures, Part I: The Evolution. Plast Reconstr Surg 2003; 112: 1125-1129.
26.Gruber RP, Friedman GD. Suture Algorithmfor the Broador BulbousNasal Tip. Plast Reconstr Surg 2002; 110: 1752-1764.
27.Gunter JP, Landecker A, Cochran CS. Frequently used grafts in rhinoplasty: nomenclature and analysis. Plast Reconstr Surg 2006;118: 14-29.
28.Vuyk HD. Suture Tip Plasty. Rhinology 1995; 33 : 30-38.
29.Byrd HS, Andochick S, Copit S,et al. Septal Extension Grafts: A Method of Controlling Tip Projection Shape. Plastic Reconstr Surg 1997;100: 999-1010.
30. Hubbard TJ. Exploiting the Septum for Maximal Tip Control. Ann Plast Surg 2000; 44: 173-180.
31. Yu MS, Jang YJ. Modified vertical dome division technique for rhinoplasty in Asian patients. Laryngoscope 2010 ;120:668-72.
32. Jang YJ, Yu MS. Rhinoplasty for the asian nose.Facial Plast Surg 2010;26:93-101.
33. Anderson JR. A Reasoned Approach to the Nasal Base. Arch Otolaryngol Head Neck Surg 1984; 110: 349-358.