Introduction
Asian nasal anatomy different form western nose. Asian nose have low nasal bridge, weak cartilages, poor nasal projection and poor tip definition. Most of the operation in Asian nose is augmentation rhinoplasty. There are many material for augmentation rhinoplasty. Autologous material that commonly used are conchal cartilage, septal cartilage, costal cartilage and dermo fat graft. Alloplastic material are Gore-Tex and silicone. Silicone implant is one of the most popular synthetic implant for augmentation rhinoplasty. The reasons are easy to shaping or carving, good for tip and dorsal augmentation and no need for harvesting. But, there are many complications from silicone augmentation rhinoplasty. The most complications are deviated implant and asymmetry. Other complications are tip and soft tissue thinning, capsular contraction. Including impending extrusion, extrusion and some infection(1),(2),(3).
Chuangsuwanich A. published complications from augmentation rhinoplasty in 548 Thai patients. Total complications rate was 6.5% (4.9% deviation, 0.7% extrusion, 0.5% hematoma and 0.3% infection)(1).
Systemic review literature from Lee MR.,et al. in management of nasal dorsum in rhinoplasty. Found alloplastic implant such as Gore-Tex and silicone showed higher complications rates. But, overall acceptable results(2).
Tham C.et al. showed 335 Chinese patients have 7.9% complications from silicone augmentation rhinoplasty. One of the reasons is form patients received largest implant volume. The overaugmentation is the main cause of extrusion and infection in augmentation rhinoplasty.
There are many methods to reduce risk of complications by used conchal cartilage as shield graft or cap graft over silicone implant to achieved good tip projection (figure1.,2.).
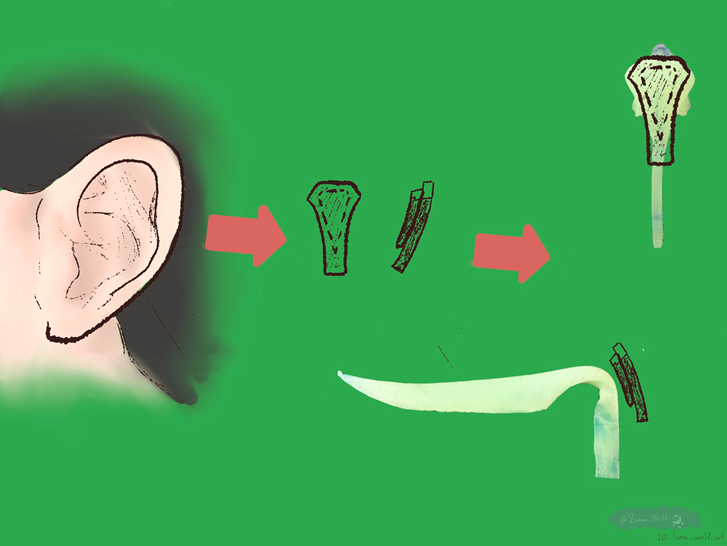
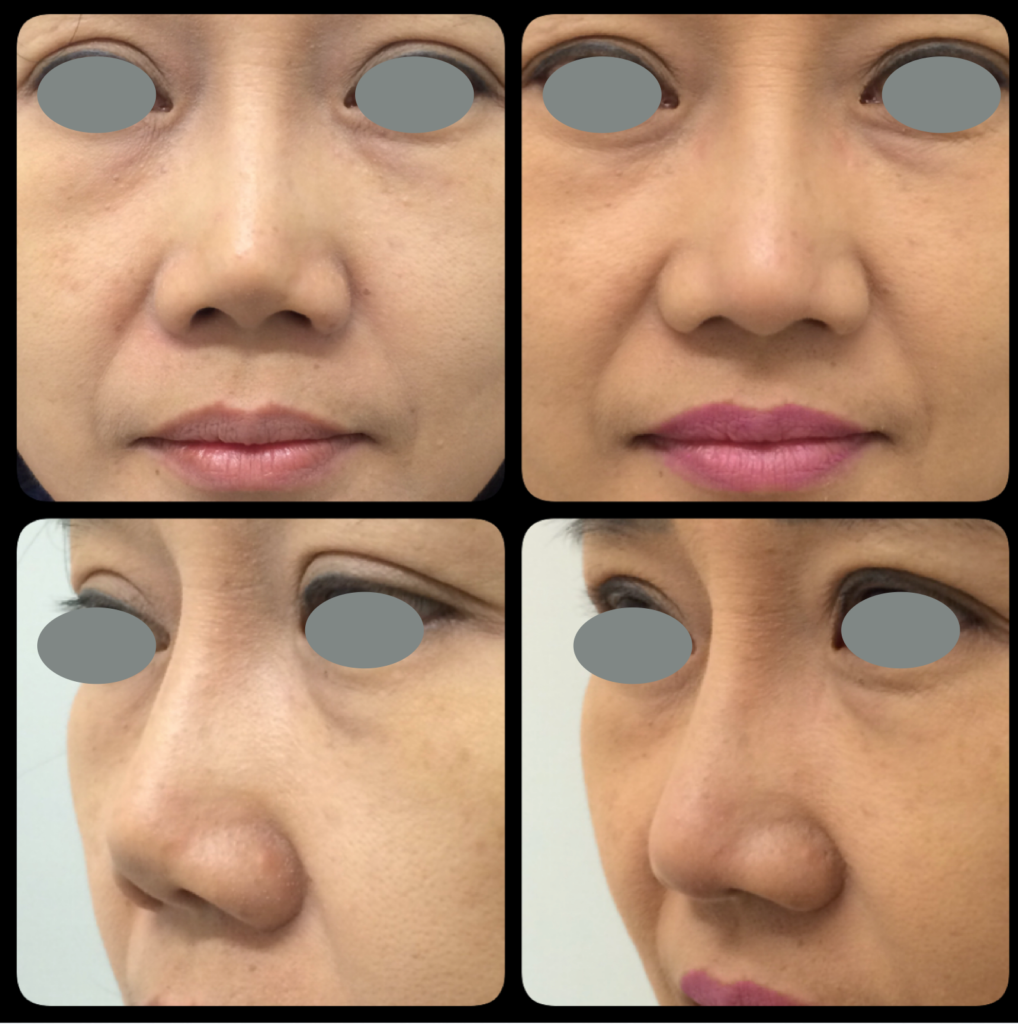
But sometime, event used conchal cartilage at tip over silicone. Form capsular contraction and not meticulously shaping cartilage graft border. There are some sharp edge border of conchal cartilage was seen when the time pass.(figure 3.)
We applied acellular dermal matrix for augmentation dorsal and tip. Acellular dermal matrix can augmented tip and dorsum with good result and low complications.

Acellular Dermal Matrix (ADM)
Acellular dermal matrix or dermal substitutes is biocompatible scaffold. From human cadaveric or porcine skin. Process to decellular and decontamination. Acellular dermal matrix are used in deep burn wound, major skin loss and reconstructive surgery including breast reconstructive surgery(4),(5).
In animal study, ADM scaffold could maintained structure and completely replaced by the host newly synthesized collagen(6).
Acellular dermal matrix can applied in rhinoplasty procedure as implant material for dorsal augmentation(7). Cover silicone implant to reduced or prevent implant visibility and capsular contraction by reduced myofibroblast activity(8).
Jackson IT.,et al. found there are no infection in 6 to 24 months post operation of ADM for palpable or irregularities of nasal dorsum in 15 patients(9). Sherris DA. study in 51 patients undergone rhinoplasty and septoplasty, no infection was reported(10).
Gryskiewicz JM.,et al. follow up for 2 years of using ADM for dorsal augmentation, tip augmentation and camouflage in 20 patients. Found 45 present of the patients had partial resorption(11).
We applied acellular dermal matrix to augmented tip projection, dorsal augmentation, cover silicone implant to camouflage implant and for corrected minor nasal deformities.
Our Experience
Setting : University hospital and private clinic.
Four facial plastic surgeons.
Start November 1st 2016 to October 31st 2017 : 192 cases.
From November 1st 2017 to October 31st 2018 : 642 cases
From November 1st 2018 to October 31st 2019 : 929 cases
Total cases 1,763 cases
Used Acellular dermal matrix for tip and dorsal augmentation rhinoplasty.
(fourteen cases used 1×5 cm. sized ADM for dorsal augmentation.)
Surgical techniques
Tip augmentation
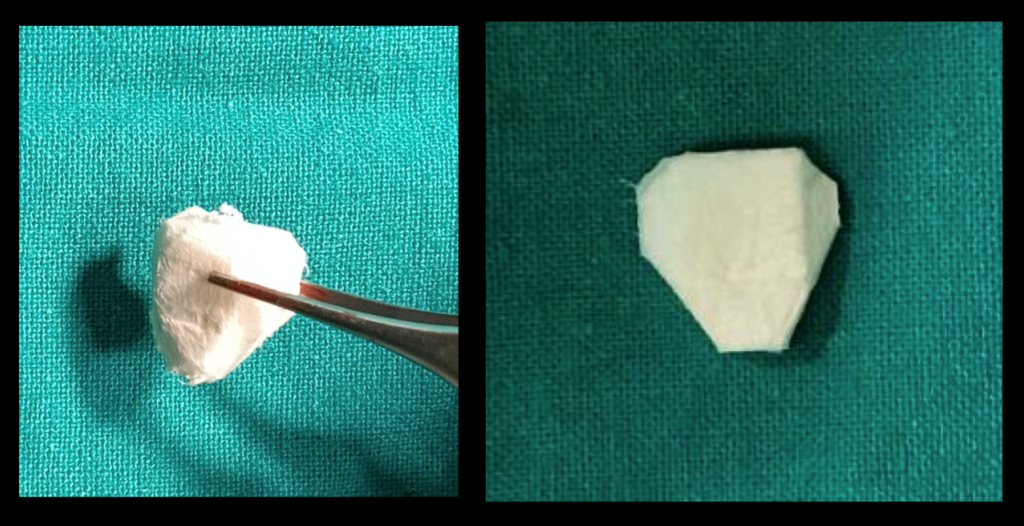
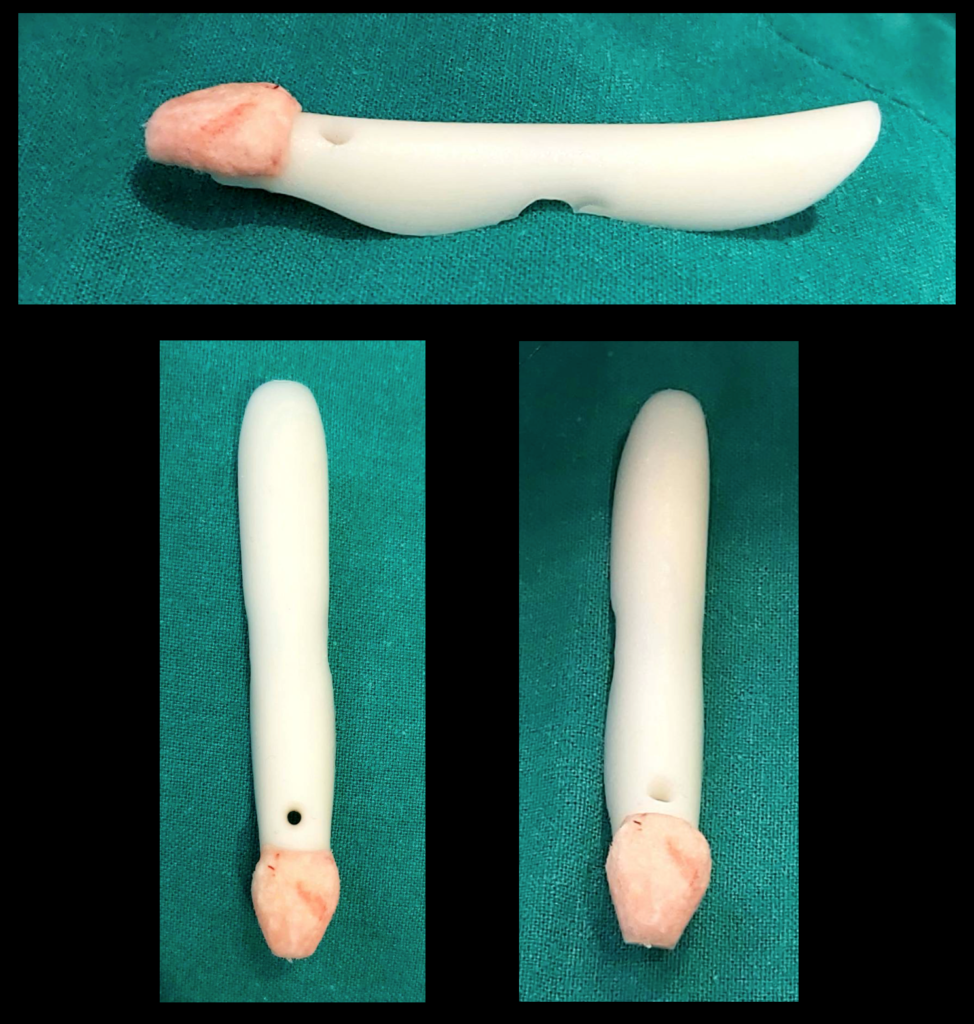
There are two type of ADM shape to augmented over silicone implant. One is carving ADM size 1×1 cm. into shield shape. (Figure 4.) (VDO1.) After carving ADM was soaked in antibiotic solution (Gentamicin 80mg/1cc.) before inserted over silicone implant or sutured with head of silicone implant using rapid vicryl 5/0.(Figure 5.)
Example of patients that used shield shape ADM size 1×1 cm. over the silicone implant are in figure 6.

In some case can used shield shape ADM size 1×1 cm. alone without silicone implant. Especially patient that need only tip augmentation. (Figure7.)
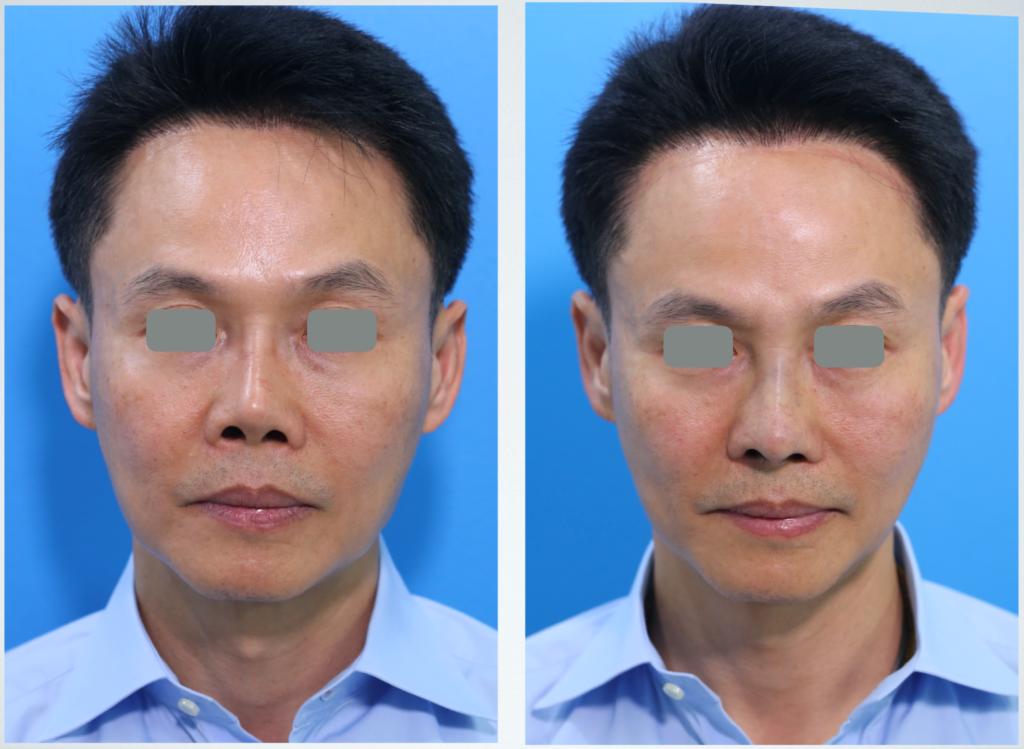
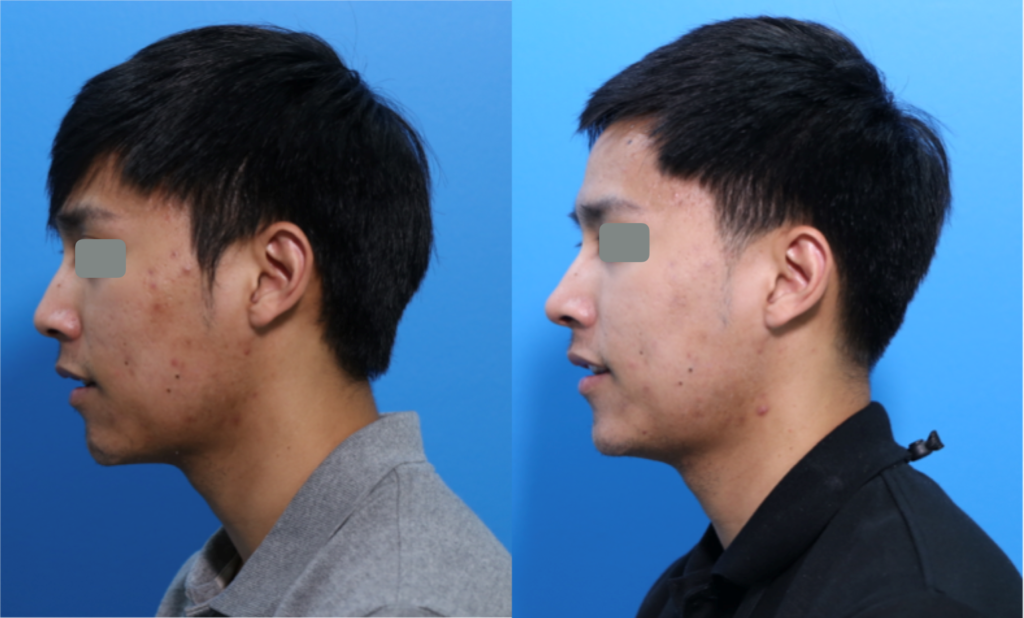
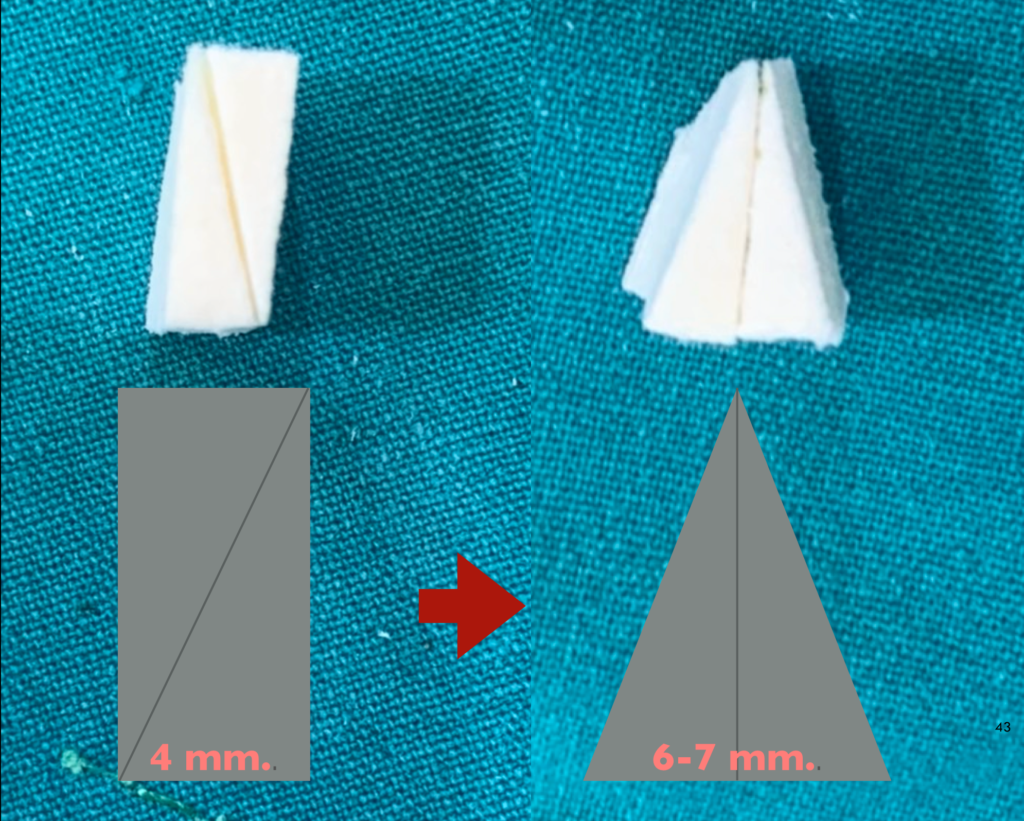
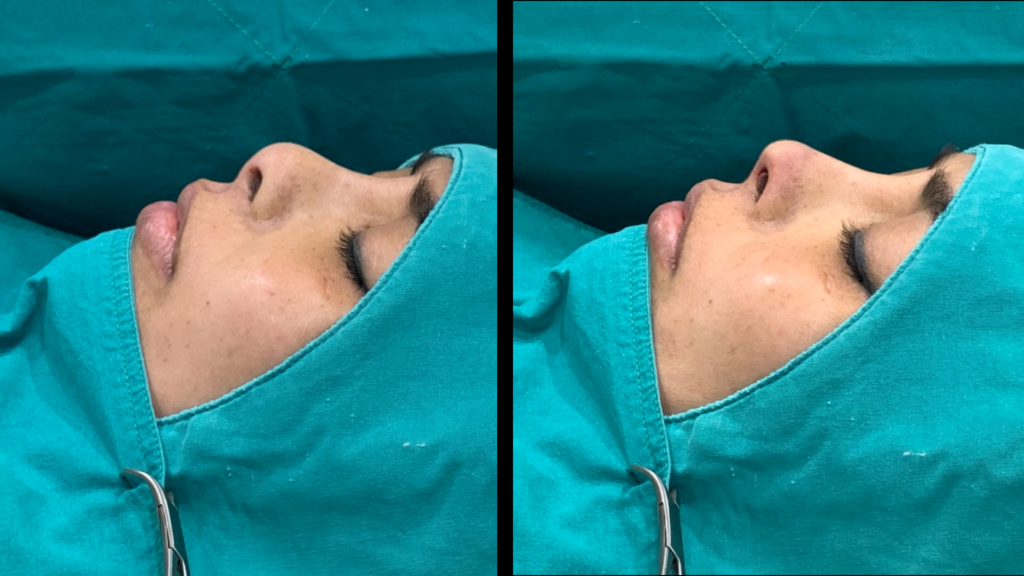
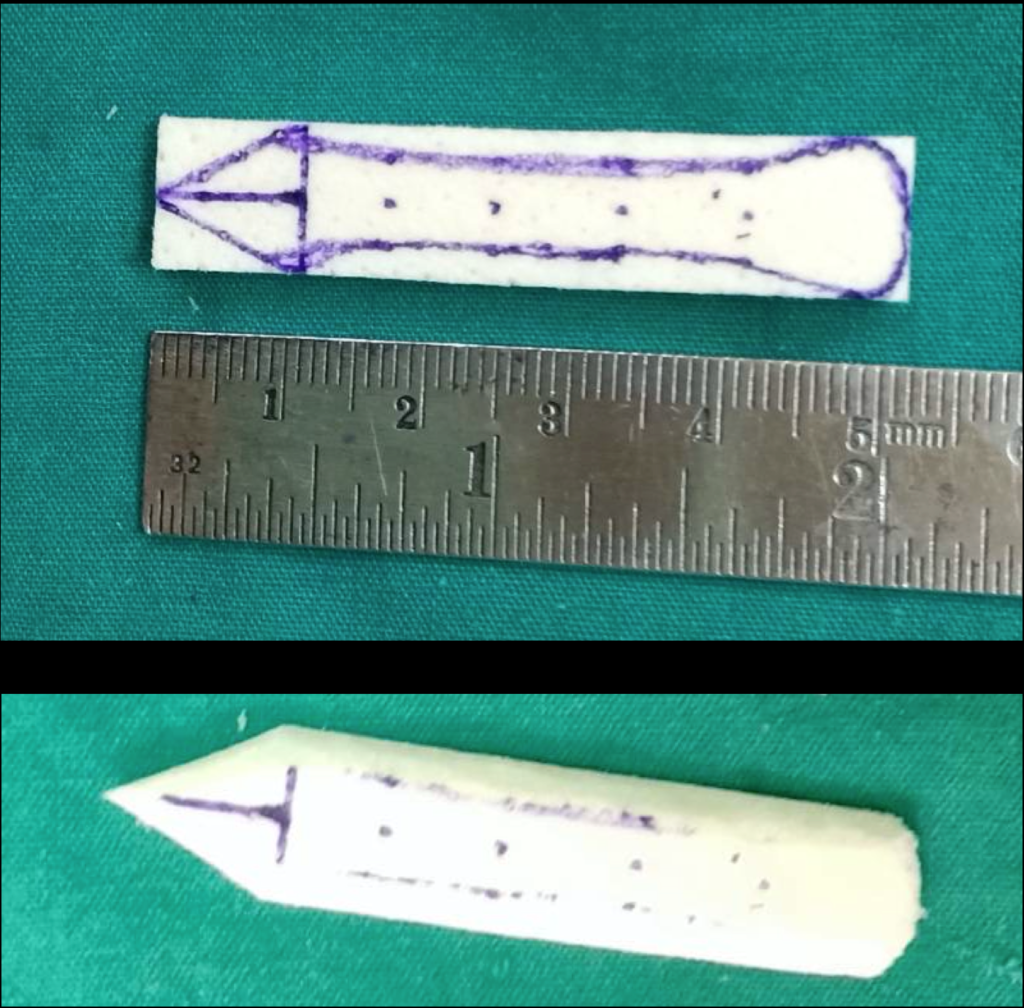
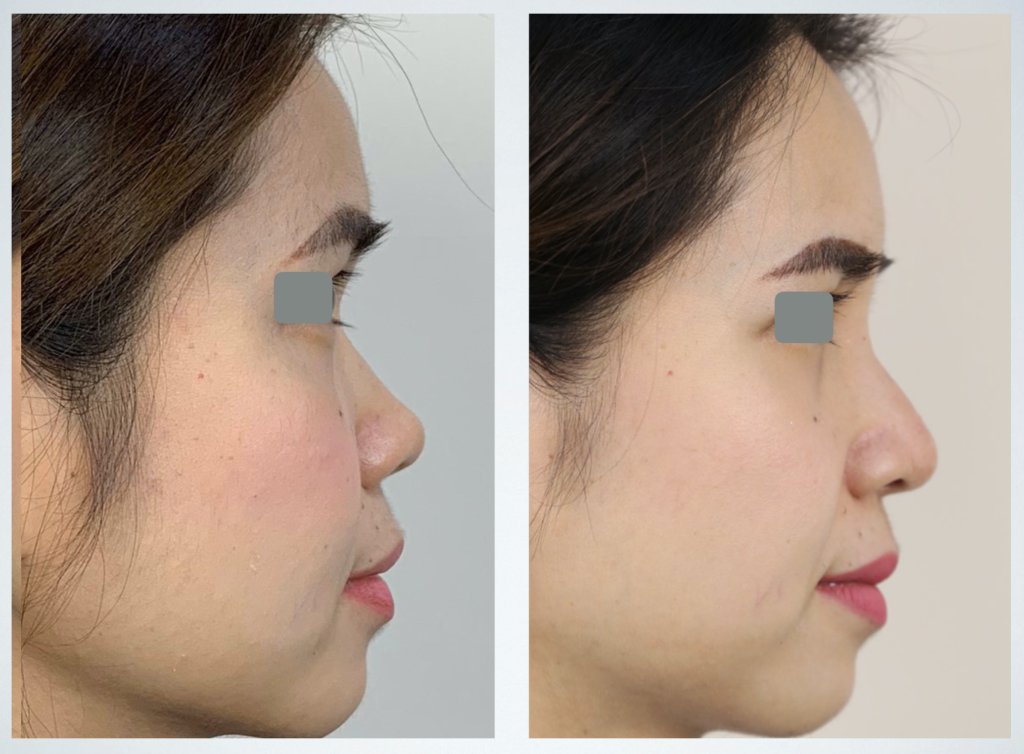
Another shape of ADM is triangular shape. By make diagonal cut on ADM size 1×1 cm. and sued together with rapid vicryl 5/0. (Figure 8.) This technique can increase thickness of ADM size 1×1 cm. form 4mm. into 6-7 mm. Then soaked in antibiotic solution and place on tip. This shape of ADM is suitable for patient have minimal nasal hump (Figure 9.1,9.2.) and need more nasal tip augmentation. (Figure 10.1,10.2)




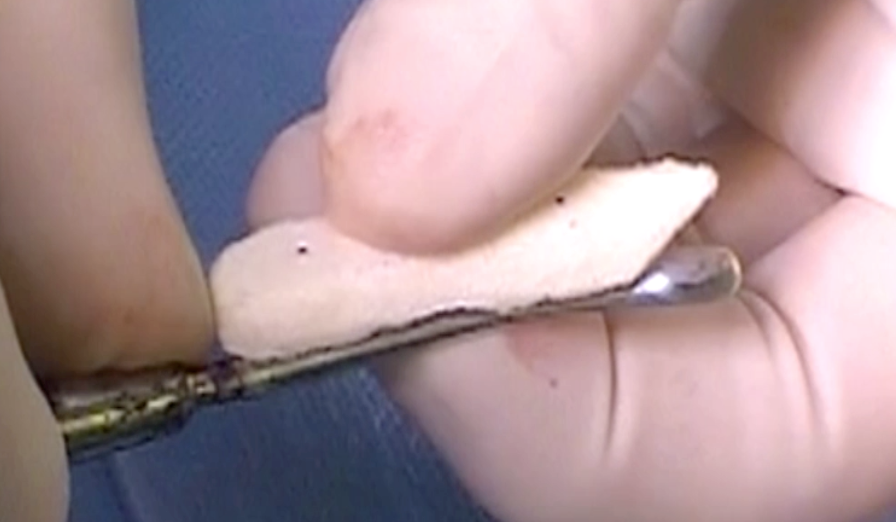
Dorsal augmentation
ADM can use as dorsal augmentation material. By applied ADM size 1cm.x5cm.x0.4cm. Design by carving or used preform type of ADM for dorsal augmentation. (Figure 11.,12.) (VDO2.) At radix area, ADM was placed in subperiosteal plane. Other part was placed in sub SMAS plane. Example of patient used dorsal and tip augmentation with ADM is figure 13.
Camouflage silicone implant
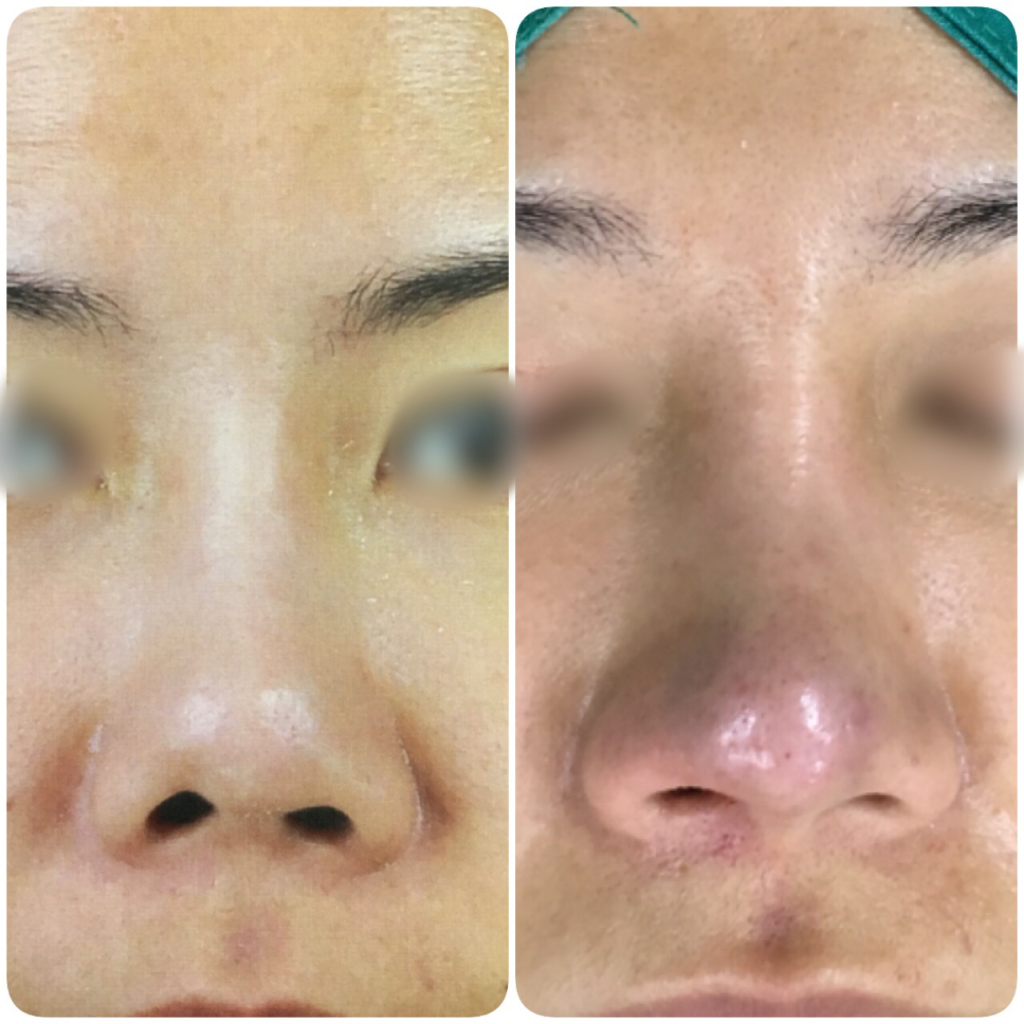
ADM can use in camouflage silicone implant in revision case that have thin skin. ADM size 1cm.x5cm.x0.4cm. was used as dorsal camouflage and ADM size 1x1cm. was used as tip augmentation and camouflage.(Figure 14.) (VDO3.) Example of patient had 14 years rhinoplasty with thin skin and obviously implant seen and post op after using ADM to camouflage dorsum and tip.(Figure 15.1,15.2)



Deformities correction
ADM can applied to correct some minor nasal and tip deformities. Both congenital and acquired deformities after trauma and post surgery. Such as thin skin with bifid nasal tip from lower lateral cartilages can camouflage with ADM size 1x1cm. (Figure 16.)
ADM. can correct or improve minor deformities after rhinoplasty surgery such as asymmetry shape, volume and contour.( Figure 17.1,17.2)


Results
One thousand seven hundred sixty three patients in this study were patients who underwent augmentation rhinoplasty at Chulalongkorn University and Fortune clinic. Operations were done between November 2016 and October 2019.
The follow up rate in 3 months is 60%. Follow up more than 6 months is 30%.
All patients were operated by the facial plastic and reconstructive surgical team, comprising four surgeons (One university teaching staff, three facial plastic surgeons in private clinic). The same technique was applied for the patients.
Complications
There are 36 patients have complications.
Minor complications : redness at tip 22 patients. Patients were treated with intravenous antibiotic for three consecutive days.
Major complications : infection 12 patients. Patients were treated by remove silicone implant and ADM. and continue intravenous antibiotic for three consecutive days.
Total resorption of ADM : there are 2 patients have total loss of ADM after a few months post operation.
Future trend
Regenerative medicine disrupted all medical field including facial plastic and reconstructive surgery. There will be a new product liked a bioactive acellular scaffold or Chondrocyte stem cell-seeded scaffold. That can induce host cell ingrowth and make scaffold permanent liked a new cartilage graft.
Conclusion
Acellular dermal matrix (ADM) is alternative material for tip and dorsal augmentation. Suitable for patients who lack of autologous graft or refuse for graft harvesting. ADM can applied for touch up operation to camouflage over autologous graft or silicone implant with harmonized tip contour. ADM have Low risk for infection. In the issue of resorption, resorption rate was need more follow up time.
Acellular dermal matrix can applied for tip augmentation, dorsal augmentation and irregularities or minor deformities camouflage with good result and low complications.
References
- Augmentation rhinoplasty with custom-made S-shape silicone implant in Asians: A 15-year experience. Chuangsuwanich A, Lohsiriwat V.,Indian J Plast Surg. 2013 Sep;46(3):533-7.
- Management of the nasal dorsum in rhinoplasty: a systematic review of the literature regarding technique, outcomes, and complications. Lee MR., Unger JG., Rorich RJ., Plast Reconstr Surg. 2011 Nov;128(5):538e-550e.
- Silicone augmentation rhinoplasty in an Oriental population. Tham C., Lai YL.,Weng CJ., CHen YR., Ann Plast Surg. 2005 Jan;54(1):1-5; discussion 6-7.
- Clinical applications of allograft skin in burn care. Wang C, Zhang F, Lineaweaver WC. Ann Plast Surg. 2020 Mar;84(3S Suppl 2):S158-S160.
- Recent advances in implant-based breast reconstruction. Colwell AS, Taylor EM. Plast Reconstr Surg. 2020 Feb;145(2):421e-432e.
- Hwang K, Hwang JH, Park JH, et al. Experimental study of autologous cartilage, acellular cadaveric dermis, lyophilized bovine pericardium and irradiated bovine tendon: applicability to nasal tip plasty. J Craniofacial Surg. 2007;18:551–558.
- Homologous tissue for dorsal augmentation. Kim CH, Park SC. Facial Plast Surg Clin North Am. 2018 Aug;26(3):311-321.
- Augmentation Rhinoplasty With Silicone Implant Covered With Acellular Dermal Matrix in Asian Noses. Such MK.,et al. J Craniofac Surg. 2017 Mar;28(2):445-448.
- Jackson IT, Yavuzer R, Silverstein P. AlloDerm for dorsal nasal irregularities. Plast Reconstr Surg. 2001;107:559–560.
- Sherris DA, Oriel BS. Human acellular dermal matrix grafts for rhinoplasty. Aesthet Surg J. 2011;31(7 Suppl):95S–100S.
- Gryskiewicz JM, Rohrich RJ, Reagan BJ. The use of alloderm for the correction of nasal contour deformities. Plast Reconstr Surg. 2001;107:561–570; discussion 571.