Abstract
Management of the osseocartilaginous vault continues to present challenges for rhinoplasty surgeons. We need to search for an atraumatic method to reshape the nasal bones in the most precise way. The author’s preference in recent years has been to seek more control and precision in osteotomies and in dorsum refinement, so as to avoid asymmetry, destabilization, and collapse of the nasal bones, palpable irregularities, residual bony spicules, and sharp edges. All these findings are very common in revision rhinoplasty, and many times caused by uncontrolled manipulation of bone, uncontrolled osteotomies, an inadequate bone refinement.
Introduction
In the past years, surgeons have begun using piezoelectric-powered ultrasonic instruments for the management of the bony vault and lateral osteotomies. [1] These devices minimize soft tissue injury, because a frequency of 25 to 29 kHz is utilized to cut bone, although a frequency greater than 50 kHz is necessary to cut neurovascular structures. Importantly, the fracture lines created by the piezotome are very accurate and eliminate the risk of radiating fracture lines encountered with traditional instrumentation. [2]
In rhinoplasty, effectiveness, precision, and safety of osteotomies are of paramount importance together with postoperative behavior (ie, ecchymosis, edema, and nasal bone healing).
This paper presents my current operative technique for modifying the osseocartilaginous vault bones based on the application of an ultrasonic piezotome, which helps to do so with preservation of nasal bone stability. This article will present the evolution of my technique, based on a single surgeon series (P.C.) of 580 cases performed over a 34 month period.
Methods
Initial Experience
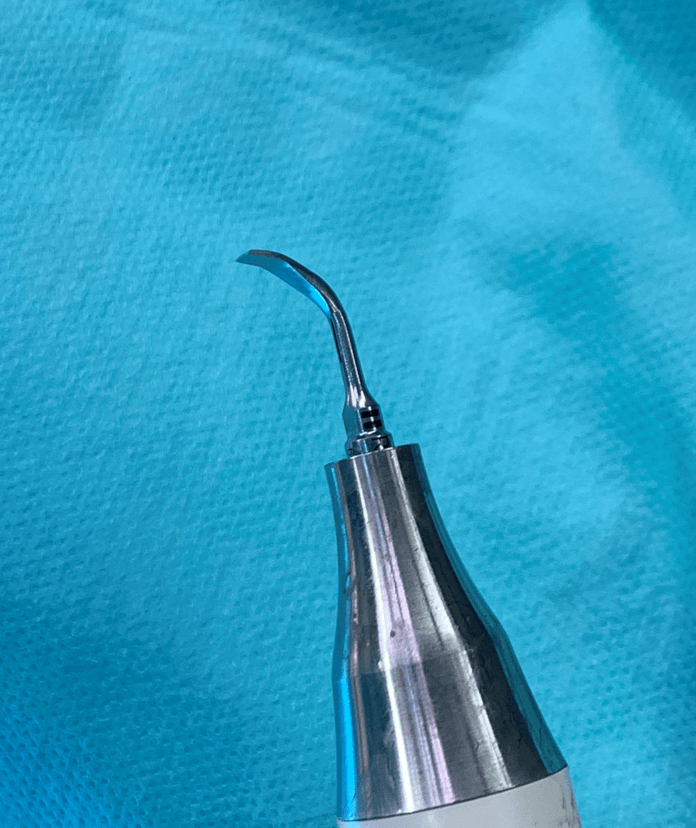
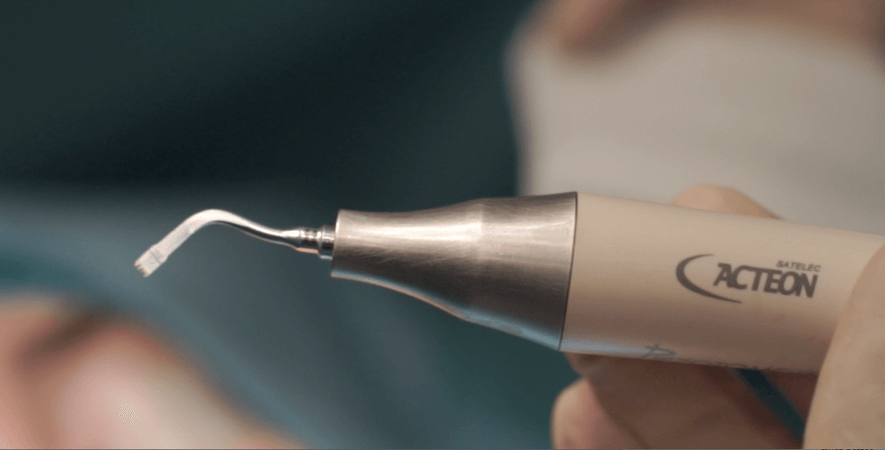
The lead author (P.C.) began using ultrasonic piezotome for rhinoplasty surgery in April 2017. Since then he has performed 580 cases. The piezotome system used for all procedures was the Piezotome Solo (Acteon Group, Mérignac, France), which has a wide variety of terminals to shape the nasal bones.
Exposure
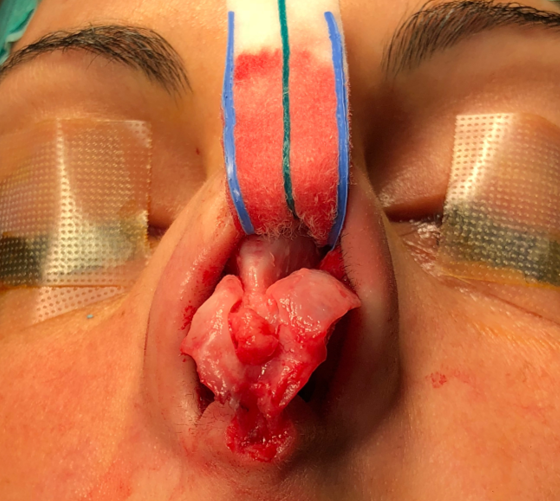
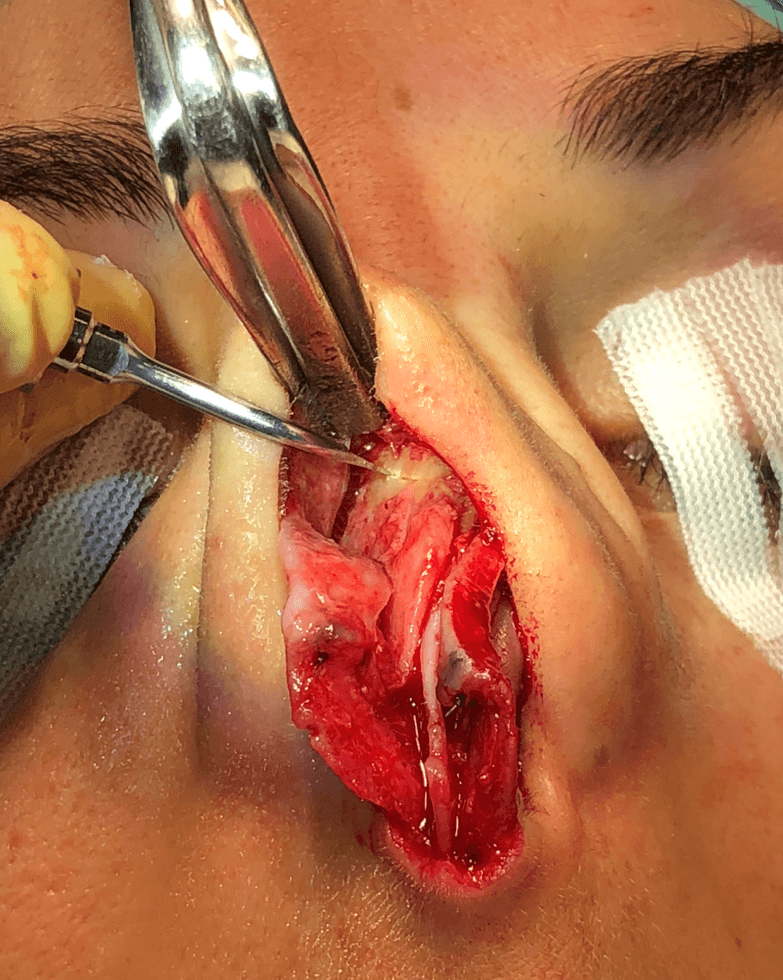
All of the operations were performed via an open approach consisting of an inverted V-shaped transcolumellar incision and infracartilaginous incisions along the caudal edges of the lower lateral cartilages. (Figure 1)
The skin and soft tissue envelope were elevated over the lower cartilages in a suprapericondrial plane, over the upper lateral cartilages (ULCs) in a suprapericondrial plane, and over the bony pyramid in the subperiosteal plane.

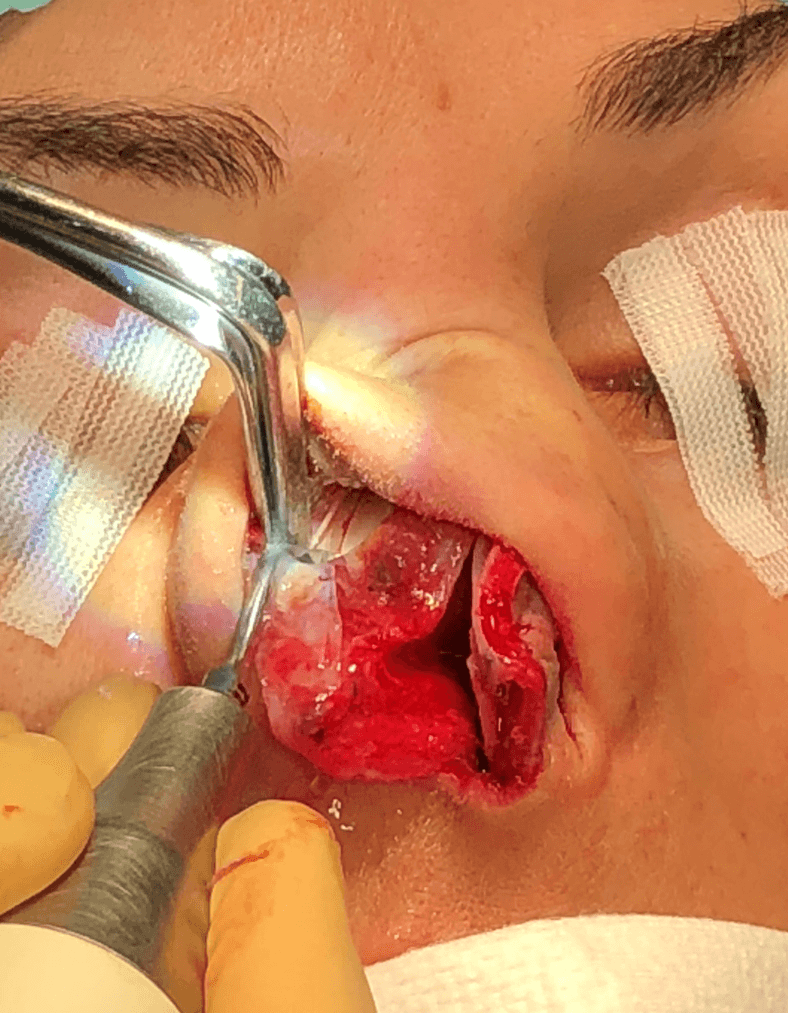
It is important to note that a full subperiosteal dissection of the bony vault needs to be performed longitudinally from the key-stone junction up to the cephalic part of the radix and transversely from one ascending frontal process of the maxilla to the other side. Usually, the lateral pyriform aperture ligaments are stretched or cut depending on their strength, to allow complete access to the nasal bony wall along the pyriform aperture. [3]
Removal of Bony-Cartilaginous Hump
Using a rasp terminal or a scraper the bony hump is removed, preserving the cartilaginous hump underneath, both the septum and the superior lateral cartilages. With this technique an open roof never occurred, because the underlying cartilages and mucosa were unharmed with the piezotome.
The cartilaginous hump will be removed later in a component separation fashion, first the septum and after the upper lateral cartilages.
Osteotomies
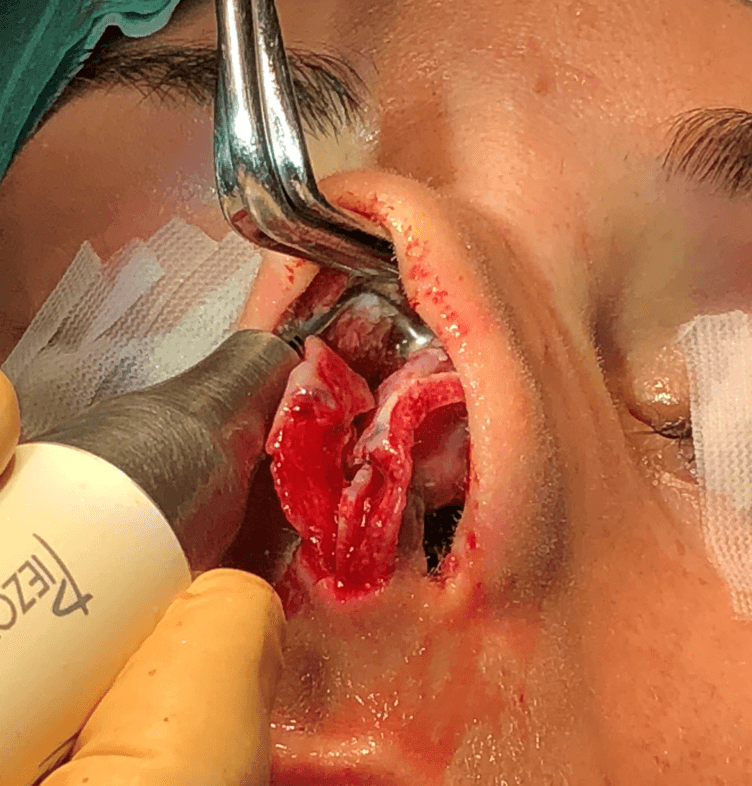
To narrow the wide bony base pyramid, a lower lateral osteotomy is performed with a straight piezo saw.
It is important to note that the lateral osteotomy is performed as low as possible, virtually always 1 to 2 mm lateral to the nasofacial groove and on the ascending portion of the frontal process of the maxilla. Usually the lead author starts above the inferior turbinate insertion, and continues in a high-low-high fashion.
After that, a medial oblique osteotomy is performed connecting to the lateral osteotomy through a little transverse osteotomy. To perform medial osteotomies, the piezotome terminal is inserted at the junction between the nasal bone and septum.
Because the piezotome does not harm the internal mucopericondrium layer, the bones are completely stable. The lead author has found that completely mobilizing the bones does not result in instability, but helps to obtain a symmetric bony pyramid.
Only in cases where the bony pyramid is really narrow and symmetric, Dr. Casas does not perfom the medial oblique osteotomy. In these cases performing only the lateral and the transverse osteotomies is enough to narrow the bony pyramid, providing great stability. This has been suggested in the great paper of Vitaly Zholtikov. [4]
In cases of crooked noses, a double lateral osteotomy is performed on the long side, and a single lateral osteotomy in the short side, always performing the medial oblique and transverse osteotomies. After this, we can infracture the convex bone and outfracture the concave bone and fix its position with the use of a long spreader graft cephalically extended to maintain its lateralized position and to visually shift the nasal centerline back to the intercanthal midpoint.
Once the osteotomies were completed, the bony edges could be smoothed with a refinement rasp terminal.
Finally, additional smoothing could be performed at the end of the surgery to reduce any irregularity palpated during the final checking.
This rhino-refinement procedure is the principal advantage of the piezotome comparing with the classic rasps and osteotomes. This refinement is performed under direct vision, so it allows the most effective, precise, and safe way to reshape the bony vault
Septoplasty
A big advantage of piezotome assisted septoplasty is the safe treatment of high septal deviations. A small strip of perpendicular plate is removed safely, without using the twisting motion of the septum. Also, there is much less risk of a radiated fracture to the skull base. [5]
Middle Third Reconstruction
After removing the bony-cartilaginous hump and doing the osteotomies, middle third reconstruction is always mandatory, in order to achieve the most beautiful and straight dorsal aesthetic lines. In my experience, spreader grafts obtained from the cartilaginous septum are the best way to do the reconstruction. We can control the width of the grafts , and therefore the width and shape of the dorsum.
Also because the bony hump was removed with the piezotome, and not an osteotome, an open roof does not exist an the upper lateral cartilages are intact, so they can be used to obtained a better middle third reconstruction.
Discussion
The adoption of new techniques in rhinoplasty surgery is sometimes difficult because of the use of new principles and changes in our technique. Four changes in operative technique and sequence are apparent2. First, extensive elevation of the soft tissue envelope allows greater visibility and assessment of the bony vault before and after surgical modification. Second, one can utilize the concept of rhinorefinement to correct asymmetries of the bony vault directly by changing the thickness of the nasal bones as well as their intrinsic convexity. Third, removal of the dorsal hump is staged with removal of the bony cap first without altering the underlying cartilaginous vault. Fourth, complete osteotomies with intact underlying periosteum/mucosa permit more precise mobilization and stabilization than previously possible.
Extensive Exposure
To utilize the piezotome for the lateral osteotomies, the surgeon must elevate the skin envelope subperiosteally from one frontal process of the maxilla across the nasal bridge to the opposite side. One of the principal advantages of this extensive exposure is the ability to visually assess the bony vault before and after osteotomies, with the latter performed under direct visualization. I have seen no disadvantages with the extensive elevation. Edema and equimosis are less than with the classical technique.
Ultrasonic Rhino-refinement
After the osteotomies, precise refinement can be achieve rasping the cephalic border of the medial oblique osteotomies. This technique allows a superior management and refinement of the K area and the transition from the bony to the cartilaginous vault. This refinement is very meticulous, and gives a much more superior control also performed under direct vision.
Trying to do this refinement with the classic rasps was dangerous, because of high risk of dettaching the nasal bones.
Bony Hump Reduction
Anatomically, the dorsal hump comprises a bony cap covering the cartilaginous vault[6]. Removal of the bony hump with an osteotome often leads to damage of the underlying cartilaginous vault or creation of an “open roof”. In contrast, the piezotome technique allows removal of the bony cap without creating an open roof or damaging the underlying upper lateral cartilages [7]. These upper lateral cartilage are used for later middle third reconstruction.
Osteotomies
Before the piezotome era, the bony vault treatment was a mystery because of limited exposure. The surgeon simply assumed that the osteotomies were symmetrical. These fracture lines very often occur at the intrinsic weak point of the lateral walls and take the path of least resistance into the open roof, which may or may not coincide with the aesthetic goal. Doing osteotomies under direct vision offers greater control and aesthetic correction of asymmetries.
My personal technique would be a lateral osteotomy, then a medial oblique osteotomy, then a transverse osteotomy to link both.
A very low lateral osteotomy can be performed under direct vision at the nasofacial groove. The medial oblique osteotomy is performed from the cephalic extent of the bony hump removal in an oblique direction reaching the lateral osteotomy with a small transverse osteotomy. These movements are much more precise and performed with visual inspection to assure that the bone moves in a specific direction to a specific extent. In cases of crooked noses, very easy double osteotomies can be performed. Overall, the surgeon has much more control over the bony vault.
Conclusions
Based on my experience, the adoption of the piezotome is easily justified, because it offers more precise analysis and surgical execution with superior results in altering the osseocartilaginous vault. With extensive exposure, one can make an accurate diagnosis of bony deformity and safely contour the nasal bones to achieve narrowing and symmetry of the bony dorsum. Stable osteotomies can be performed under direct vision with precise mobilization and control. Therefore, the upper third of the rhinoplasty operation is much better managed.
[1] Robiony M, Polini F, Costa F, et al. Ultrasound piezoelec- tric vibrations to perform osteotomies in rhinoplasty. J Oral Maxillofac Surg. 2007;65(5):1035-1038.
[2] Gerbault O, Daniel RK, Kosins AM. The role of piezoelectric instrumentation in rhinoplasty surgery. Aesthet Surg J. 2016;36(1):21-34.
[3] Daniel RK, Pálházi P. Rhinoplasty: An Anatomical and Clinical Atlas. Cham, Switzerland: Springer International Publishing AG; 2018.
[4] Zholtikov V, Golovatinsky V, Palhazi P et al. Rhinoplasty: A Sequential Approach to Managing the Bony Vault. Aesthet Surg J. 2019 Jun 3. pii: sjz158.
[5] Gerbault O, Daniel RK, Palhazi P etr al. Reassessing Surgical Management of the Bony Vault in Rhinoplasty. Aesthet Surg J. 2018 May 15;38(6):590-602.
[6] Palhazi P, Daniel RK, Kosins AM. The osseocartilaginous vault of the nose: anatomy and surgical observations. Aesthet Surg J. 2015;35:242-251.
[7] Rohrich RJ, Minoli JJ, Adams WP ert al. The lateral nasal osteotomy in rhinoplasty: an anatomic endoscopic comparison of the external versus the internal approach. Plast Reconstr Surg. 1997;99(5):1309-1312; discussion 1313.