Introduction:
The nasal dorsum is often narrowed during rhinoplasty as a result of open roof closure following reduction of the nasal dorsum. In the presence of an open roof, medial and lateral osteotomies, or lateral osteotomies alone, allow medial displacement of the nasal bones into the newly created paramedian space of the open roof. The cartilaginous dorsum is narrowed as upper lateral cartilages are approximated to the narrower portion of the cartilage exposed after reduction of the cartilaginous dorsum. In rhinoplasty procedures not requiring dorsum reduction, however, the paramedian spaces resulting from dorsum reduction do not exist. In such cases, a removal of wedges of bone and cartilage adjacent to the center of the bony dorsum and midline of the septal cartilage is necessary. A variation of this procedure, involving only the middle (cartilagenous) vault, has been termed the “reverse spreader” technique due to its converse anatomical basis to spreader grafts (1). This chapter describes the indications, anatomical, and procedural details of the “extended reverse spreader” technique to narrow the entire nasal dorsum width when profile reduction of the dorsum is undesired.
Anatomical considerations:
In review, the nasal bones serve as the structural support of the upper nasal vault. The bony nasal vault is comprised of the paired nasal bones, the nasal processes of the frontal bones, and the nasal processes of the maxillary bones. The width of the nasal dorsum resembles the arch of an A-frame structure created by the shape of the nasal bones.
The cartilagenous nasal dorsum is comprised of the paired upper lateral cartilages and their junction with the ventral portion of the quadrangular cartilage of the septum. The quadrangular cartilage is flared at its ventral portion where the upper lateral cartilages attach paramedian to the midline of the nasal dorsum (figure 1). This flared or wider portion of the quadrangular cartilage plays an important role in the maintenance of an appropriate angle between the quadrangular cartilage and the upper lateral cartilages. This area, known as the internal nasal valve, is among the most significant functional areas of the nose. The ventral flare of the quadrangular cartilage is also aesthetically important in determining the width of the middle nasal vault. A narrow flare at this portion of the quadrangular cartilage results in a narrower middle vault, while a wider flare results in a wider middle vault (2,3).
Surgical techniques in rhinoplasty must be individually tailored to meet the aesthetic and functional needs of each patient. The extended reverse spreader technique is indicated in a nose that is wide from the root to the supratip area with satisfactory dorsum that is appropriately projected with adequate internal valve function.

Surgical technique:
The procedure may be preformed under monitored sedation anesthesia or general anesthesia depending on the preferences of the surgeon and patient. While the techniques used may be applied via endonasal or external approaches, the author favors the improved visibility offered by the external approach.
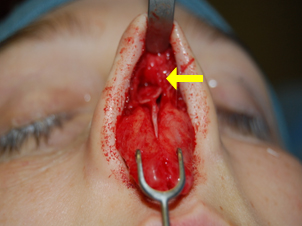
Once the transcolumellar and marginal incisions are completed, the skin-soft-tissue envelope (SSTE) is elevated off of the lower lateral cartilages, and ventral middle vault in the subperichondrial plane. The SSTE is then elevated off of the bony dorsum in the subperiostial plane. The caudal septum is exposed along both sides using subperichondrial elevation of the mucoperiostium, and the dissection is carried along the ventral portion of the quadrangular cartilage. The upper lateral cartilage and the quadrangular cartilage are separated bilaterally, preserving the flared portion of the quadrangular cartilage.
At this point the desired amount of narrowing is re-assessed, and markings are made. Wedges of cartilage are removed from the paramedian flared portions of the ventral quadrangular cartilage using an 11-blade. Tapered wedges of bone are removed from the pareamedian portion of the bony dorsum using a 2mm osteotome bilaterally. This step creates an open roof without reduction of nasal dorsum projection. The resulting composite open roof affords medial displacement of the nasal bones and upper lateral cartilages. Medial and lateral osteotomies are then performed. The medial osteotomies are performed from the rostral extent of the open roof on each side. The lateral osteotomies are preformed via mucosal incisions in the nasal vestibule, although other lateral osteotomy techniques such as perforating external osteotomies may be considered according to surgeon preference.
Once the nasal bones are medialized, the upper lateral cartilages are re-approximated with the quadrangular cartilage along the dorsum using 5-0 pds or prolene suture in mattress fashion. The tip is then treated accordingly. The SSTE is replaced and incisions are closed according to surgeon preference. The nasal dorsum is dressed with steri-strips and a thermoplastic splint.
Results:
Case #1


Case #1: This is a 23 year-old female who requested rhinoplasty to reduce dorsum width without deprojection of the dorsal profile. The patient was treated with external rhinoplasty approach to perform the extended spreader graft procedure, and tip rhinoplasty. Her results show balanced reduction of the width of the dorsum with complete retention of the dorsal profile.
Case #2


Case #2: This is a 20 year-old female requesting reduction of dorsal width with maintenance of dorsum profile features. External rhinoplasty with extended spreader technique was performed. The results depict appropriate and balanced reduction of nasal dorsum width and maintenance of dorsum profile projection.
Discussion:
Narrowing of the nasal dorsum after dorsal hump or profile reduction may be inherent in closure of the open roof. Most commonly, as the dorsal profile is reduced the remaining anatomical structures are narrower than the native nasal dorsum. In patients with wide dorsum not requiring reduction of the nasal dorsal profile, however, a physical narrowing of the nasal dorsum requires reduction of the width of the dorsal flare of the septum in addition to paramedian reduction of nasal bone width. It is the author’s belief that combination of these two narrowing procedures affords greater efficacy of medial and lateral osteotomies in narrowing the nasal dorsum. The “reverse spreader” technique described above is a valuable complement to the armamentarium of the experienced rhinoplasty surgeon.
References:
- Prendiville S, Zimbler MS, Kokoska MS, Thomas JR, Middle-Vault Narrowing in the Wide Nasal Dorsum The “Reverse Spreader” Technique, Arch Facial Plast Surg. 2002;4:52-55
- Teller DC, Anatomy of a rhinoplasty: emphasis on the middle third of the nose, Facial Plast Surg. 1997 Oct;13(4):241-52
- Fischer H, Gubisch W, Nasal Valves-Importance and Surgical Procedures Facial plast Surg 2006; 22(4): 266-280